van Peet Petra G, Gussekloo Jacobijn, den Elzen Wendy P J, Blom Jeanet W, de Waal Margot W M, de Ruijter Wouter
a Department of Public Health and Primary Care , Leiden University Medical Center , Leiden , The Netherlands.
Scand J Prim Health Care. 2015;33(4):260-8. doi: 10.3109/02813432.2015.1117281.
To assess the influence vulnerability and severity of cardiovascular disease (CVD), on prescription rates of secondary cardiovascular preventive drugs in old age.
Population-based observational study within the ISCOPE study.
General practices in the Netherlands.
A total of 1350 patients with a history of CVD (median age 81 years, 50% female).
One-year prescription rates of lipid-lowering drugs and antithrombotics were obtained from the electronic medical records of 46 general practitioners (GPs). Prescription of both drugs for ≥ 270 days per year was considered optimal. GPs made a judgement of vulnerability. Severity of CVD was expressed as major (myocardial infarction, stroke, or arterial surgery) versus minor (angina, transient ischaemic attack, or claudication).
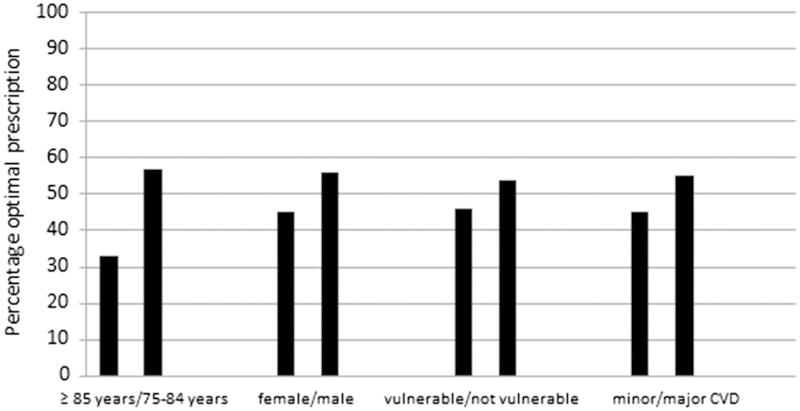
GPs considered 411 (30%) participants to be vulnerable and 619 (55%) participants had major CVD. Optimal treatment was prescribed to 680 (50%) participants, whereas 370 (27%) received an antithrombotic drug only, 53 (4%) a lipid-lowering drug only, and 247 (18%) received neither. Optimal treatment was lower in participants aged ≥ 85 years (OR 0.37 [95% CI 0.29-0.48]), in females (OR 0.63 [0.50-0.78]), in vulnerable persons (OR 0.79 [0.62-0.99]) and in participants with minor CVD (OR 0.65 [0.53-0.81]). Multivariate ORs remained similar whereas vulnerability lost its significance (OR 0.88 [0.69-1.1]).
In old age, GPs' judgement of vulnerability is not independently associated with lower treatment rates of both lipid-lowering drugs and antithrombotics, whereas a history of minor CVD is. Individual proactive re-evaluation of preventive treatment in older (female) patients, especially those with a history of minor CVD, is recommended. Key points Prescriptions of lipid-lowering drugs and antithrombotics in secondary cardiovascular prevention tend to decline with age. In this study with median age 81 years, 50% of participants received optimal treatment with both lipid-lowering drugs and antithrombotics. GPs' judgement of vulnerability was not independently associated with optimal treatment. A history of less severe cardiovascular disease was independently associated with lower prescription rates of lipid-lowering drugs and antithrombotics. Proactive individual re-evaluation of cardiovascular preventive treatment in older (female) patients, especially patients with less severe cardiovascular disease, is recommended.
评估心血管疾病(CVD)的易损性和严重程度对老年患者二级心血管预防药物处方率的影响。
ISCOPE研究中的基于人群的观察性研究。
荷兰的全科医疗诊所。
共有1350例有CVD病史的患者(中位年龄81岁,50%为女性)。
从46名全科医生(GP)的电子病历中获取降脂药物和抗血栓药物的一年处方率。每年两种药物处方≥270天被视为最佳。全科医生对易损性进行了判断。CVD的严重程度分为重度(心肌梗死、中风或动脉手术)和轻度(心绞痛、短暂性脑缺血发作或跛行)。
全科医生认为411名(30%)参与者易损,619名(55%)参与者患有重度CVD。680名(50%)参与者接受了最佳治疗,而370名(27%)仅接受了抗血栓药物治疗,53名(4%)仅接受了降脂药物治疗,247名(18%)两种药物都未接受。85岁及以上的参与者(比值比[OR]0.37[95%置信区间(CI)0.29 - 0.48])、女性(OR 0.63[0.50 - 0.78])、易损人群(OR 0.79[0.62 - 0.99])和患有轻度CVD的参与者(OR 0.65[0.53 - 0.81])接受最佳治疗的比例较低。多变量OR值保持相似,而易损性失去了显著性(OR 0.88[0.69 - 1.1])。
在老年患者中,全科医生对易损性的判断与降脂药物和抗血栓药物的较低治疗率无独立相关性,而轻度CVD病史则与之相关。建议对老年(女性)患者,尤其是有轻度CVD病史的患者,进行个体预防性治疗的主动重新评估。要点:二级心血管预防中降脂药物和抗血栓药物的处方率往往随年龄下降。在这项中位年龄为81岁的研究中,50%的参与者接受了降脂药物和抗血栓药物的最佳治疗。全科医生对易损性的判断与最佳治疗无独立相关性。较轻的心血管疾病病史与降脂药物和抗血栓药物的较低处方率独立相关。建议对老年(女性)患者,尤其是心血管疾病较轻的患者,进行心血管预防性治疗的主动个体重新评估。