Oxborough David, Ghani Saqib, Harkness Allan, Lloyd Guy, Moody William, Ring Liam, Sandoval Julie, Senior Roxy, Sheikh Nabeel, Stout Martin, Utomi Victor, Willis James, Zaidi Abbas, Steeds Richard
Research Institute for Sports and Exercise Sciences, Liverpool John Moores University , Liverpool, L3 9UT , UK.
Department of Cardiology, Southend University Hospital NHS Trust , Westcliffe on Sea , UK.
Echo Res Pract. 2014 Sep 1;1(1):1-9. doi: 10.1530/ERP-14-0004. Epub 2014 May 6.
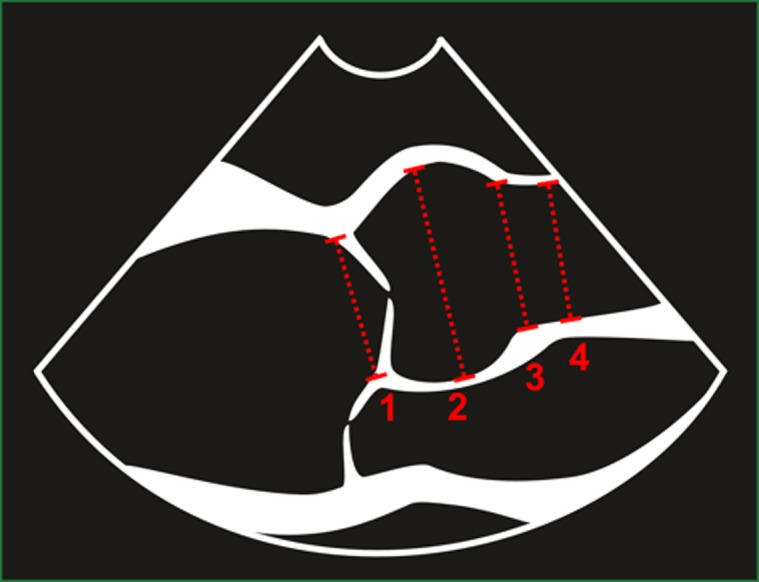
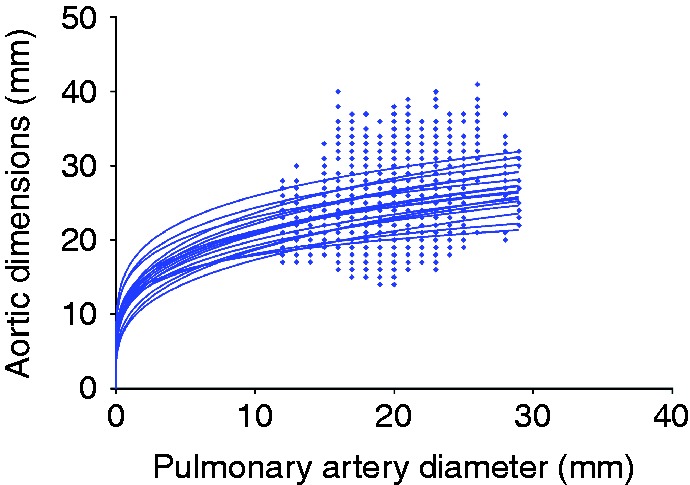
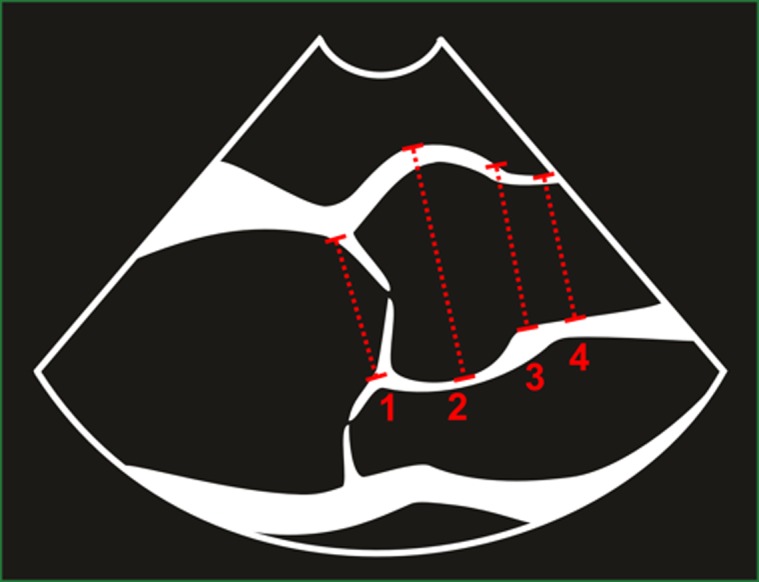
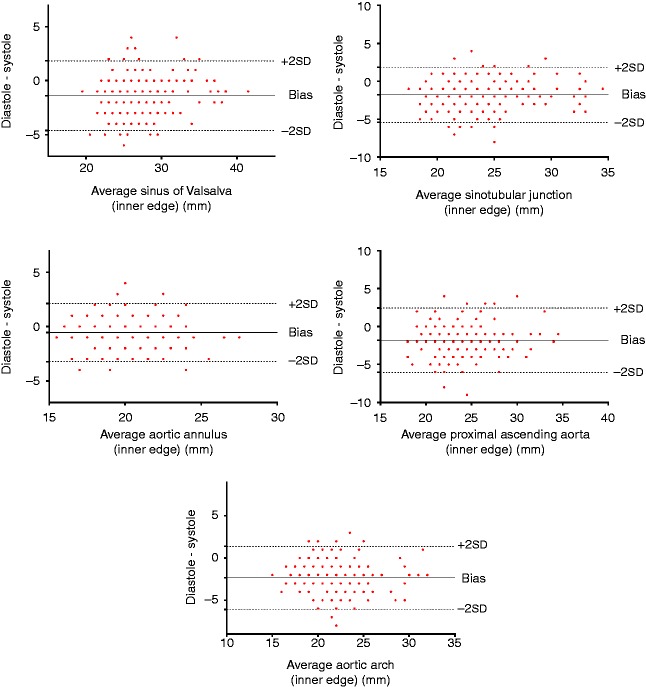
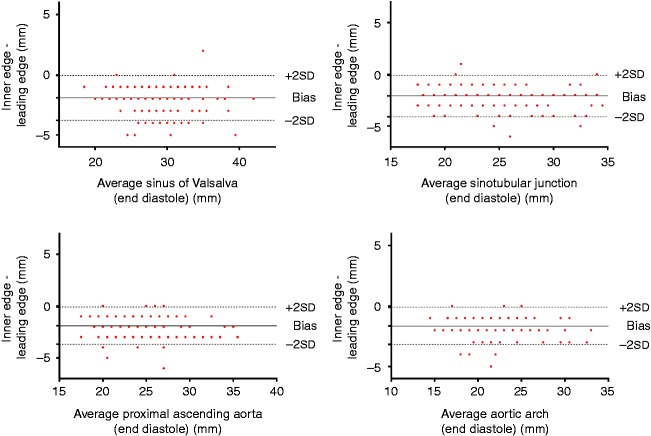
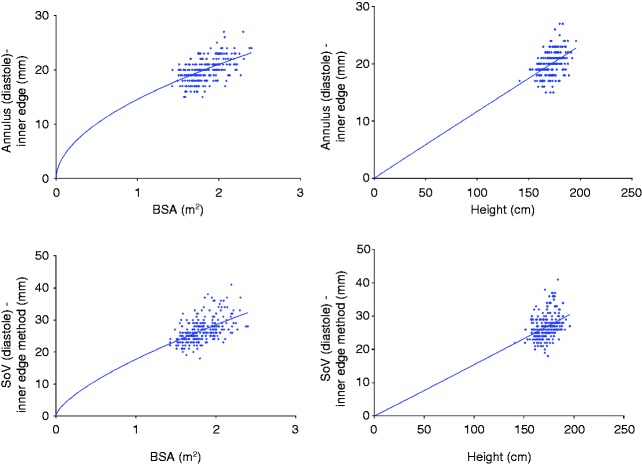
The aim of the study is to establish the impact of 2D echocardiographic methods on absolute values for aortic root dimensions and to describe any allometric relationship to body size. We adopted a nationwide cross-sectional prospective multicentre design using images obtained from studies utilising control groups or where specific normality was being assessed. A total of 248 participants were enrolled with no history of cardiovascular disease, diabetes, hypertension or abnormal findings on echocardiography. Aortic root dimensions were measured at the annulus, the sinus of Valsalva, the sinotubular junction, the proximal ascending aorta and the aortic arch using the inner edge and leading edge methods in both diastole and systole by 2D echocardiography. All dimensions were scaled allometrically to body surface area (BSA), height and pulmonary artery diameter. For all parameters with the exception of the aortic annulus, dimensions were significantly larger in systole (P<0.05). All aortic root and arch measurements were significantly larger when measured using the leading edge method compared with the inner edge method (P<0.05). Allometric scaling provided a b exponent of BSA(0.6) in order to achieve size independence. Similarly, ratio scaling to height in subjects under the age of 40 years also produced size independence. In conclusion, the largest aortic dimensions occur in systole while using the leading edge method. Reproducibility of measurement, however, is better when assessing aortic dimensions in diastole. There is an allometric relationship to BSA and, therefore, allometric scaling in the order of BSA(0.6) provides a size-independent index that is not influenced by the age or gender.
本研究的目的是确定二维超声心动图方法对主动脉根部尺寸绝对值的影响,并描述其与身体大小的任何异速生长关系。我们采用了全国性横断面前瞻性多中心设计,使用从有对照组的研究或评估特定正常情况的研究中获取的图像。共有248名无心血管疾病、糖尿病、高血压病史且超声心动图检查无异常发现的参与者入组。通过二维超声心动图,在舒张期和收缩期使用内缘法和前缘法测量主动脉根部在瓣环、主动脉窦、窦管交界处、升主动脉近端和主动脉弓处的尺寸。所有尺寸均根据身体表面积(BSA)、身高和肺动脉直径进行异速生长缩放。除主动脉瓣环外,所有参数在收缩期的尺寸均显著更大(P<0.05)。与内缘法相比,使用前缘法测量时,所有主动脉根部和弓部的测量值均显著更大(P<0.05)。为了实现尺寸独立性,异速生长缩放得出BSA的b指数为0.6。同样,40岁以下受试者按身高进行比例缩放也能实现尺寸独立性。总之,使用前缘法时,主动脉最大尺寸出现在收缩期。然而,在舒张期评估主动脉尺寸时测量的可重复性更好。与BSA存在异速生长关系,因此,按BSA(0.6)顺序进行异速生长缩放可提供一个不受年龄或性别影响的尺寸独立指数。