Lee Jang Hoon, Bae Myung Hwan, Yang Dong Heon, Park Hun Sik, Cho Yongkeun, Lee Won Kee, Jeong Myung Ho, Kim Young Jo, Cho Myeong Chan, Kim Chong Jin, Chae Shung Chull
Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
Department of Preventive Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
Korean J Intern Med. 2016 Mar;31(2):267-76. doi: 10.3904/kjim.2014.268. Epub 2015 Dec 23.
BACKGROUND/AIMS: Angiotensin II type 1 receptor blockers (ARBs) have not been adequately evaluated in patients without left ventricular (LV) dysfunction or heart failure after acute myocardial infarction (AMI).
Between November 2005 and January 2008, 6,781 patients who were not receiving angiotensin-converting enzyme inhibitors (ACEIs) or ARBs were selected from the Korean AMI Registry. The primary endpoints were 12-month major adverse cardiac events (MACEs) including death and recurrent AMI.
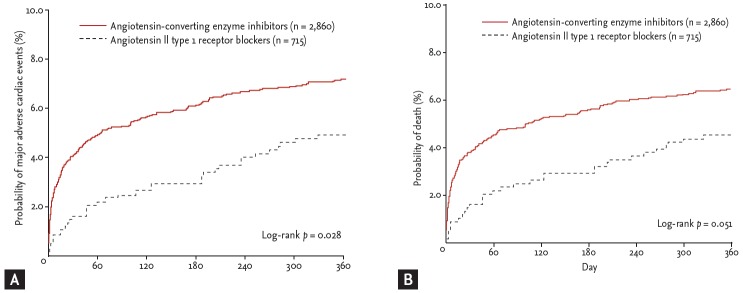
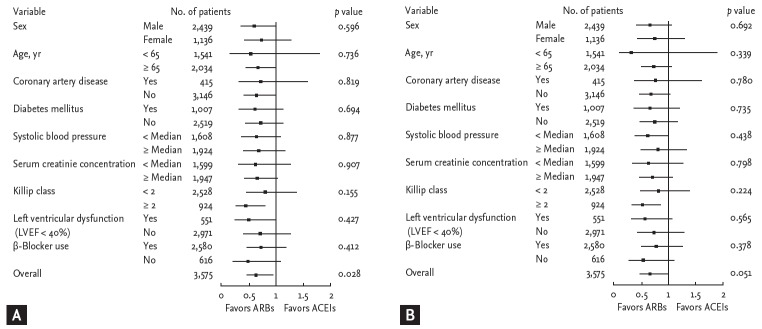
Seventy percent of the patients were Killip class 1 and had a LV ejection fraction ≥ 40%. The prescription rate of ARBs was 12.2%. For each patient, a propensity score, indicating the likelihood of using ARBs during hospitalization or at discharge, was calculated using a non-parsimonious multivariable logistic regression model, and was used to match the patients 1:4, yielding 715 ARB users versus 2,860 ACEI users. The effect of ARBs on in-hospital mortality and 12-month MACE occurrence was assessed using matched logistic and Cox regression models. Compared with ACEIs, ARBs significantly reduced in-hospital mortality(1.3% vs. 3.3%; hazard ratio [HR], 0.379; 95% confidence interval [CI], 0.190 to0.756; p = 0.006) and 12-month MACE occurrence (4.6% vs. 6.9%; HR, 0.661; 95% CI, 0.457 to 0.956; p = 0.028). However, the benefit of ARBs on 12-month mortality compared with ACEIs was marginal (4.3% vs. 6.2%; HR, 0.684; 95% CI, 0.467 to 1.002; p = 0.051).
Our results suggest that ARBs are not inferior to, and may actually be better than ACEIs in Korean patients with AMI.
背景/目的:血管紧张素II 1型受体阻滞剂(ARB)在急性心肌梗死(AMI)后无左心室(LV)功能障碍或心力衰竭的患者中尚未得到充分评估。
2005年11月至2008年1月期间,从韩国AMI注册中心选取6781例未接受血管紧张素转换酶抑制剂(ACEI)或ARB的患者。主要终点为12个月主要不良心脏事件(MACE),包括死亡和再发AMI。
70%的患者为Killip 1级,左心室射血分数≥40%。ARB的处方率为12.2%。对于每位患者,使用非简约多变量逻辑回归模型计算一个倾向评分,该评分表明住院期间或出院时使用ARB的可能性,并用于将患者按1:4匹配,产生715例ARB使用者和2860例ACEI使用者。使用匹配的逻辑回归和Cox回归模型评估ARB对住院死亡率和12个月MACE发生的影响。与ACEI相比,ARB显著降低了住院死亡率(1.3%对3.3%;风险比[HR],0.379;95%置信区间[CI],0.190至0.756;p = 0.006)和12个月MACE的发生(4.6%对6.9%;HR,0.661;95%CI,0.457至0.956;p = 0.028)。然而,与ACEI相比,ARB对12个月死亡率的益处微乎其微(4.3%对6.2%;HR,0.684;95%CI,0.467至1.002;p = 0.051)。
我们的结果表明,在韩国AMI患者中,ARB并不劣于ACEI,实际上可能更好。