Lerario Michael P, Gialdini Gino, Lapidus Daniel M, Shaw Mesha M, Navi Babak B, Merkler Alexander E, Lip Gregory Y H, Healey Jeff S, Kamel Hooman
Department of Neurology, Weill Cornell Medical College, New York, NY, United States of America.
Feil Family Brain and Mind Research Institute, Weill Cornell Medical College, New York, NY, United States of America.
PLoS One. 2015 Dec 23;10(12):e0145579. doi: 10.1371/journal.pone.0145579. eCollection 2015.
We aimed to estimate the risk of ischemic stroke after intracranial hemorrhage in patients with atrial fibrillation.
Using discharge data from all nonfederal acute care hospitals and emergency departments in California, Florida, and New York from 2005 to 2012, we identified patients at the time of a first-recorded encounter with a diagnosis of atrial fibrillation. Ischemic stroke and intracranial hemorrhage were identified using validated diagnosis codes. Kaplan-Meier survival statistics and Cox proportional hazard analyses were used to evaluate cumulative rates of ischemic stroke and the relationship between incident intracranial hemorrhage and subsequent stroke.
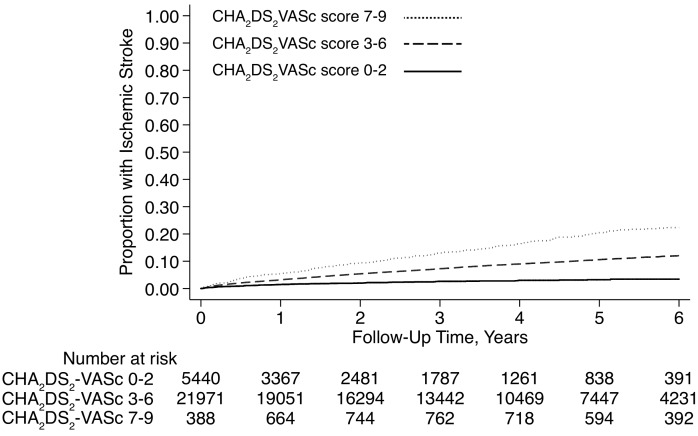
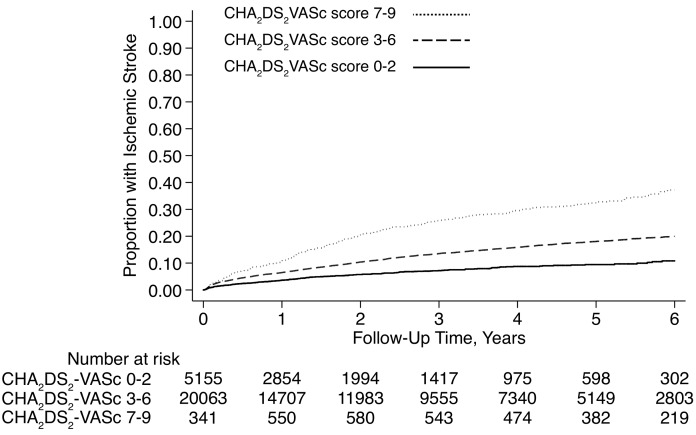
Among 2,084,735 patients with atrial fibrillation, 50,468 (2.4%) developed intracranial hemorrhage and 89,594 (4.3%) developed ischemic stroke during a mean follow-up period of 3.2 years. The 1-year cumulative rate of stroke was 8.1% (95% CI, 7.5-8.7%) after intracerebral hemorrhage, 3.9% (95% CI, 3.5-4.3%) after subdural hemorrhage, and 2.0% (95% CI, 2.0-2.1%) in those without intracranial hemorrhage. After adjustment for the CHA2DS2-VASc score, stroke risk was elevated after both intracerebral hemorrhage (hazard ratio [HR], 2.8; 95% CI, 2.6-2.9) and subdural hemorrhage (HR, 1.6; 95% CI, 1.5-1.7). Cumulative 1-year rates of stroke ranged from 0.9% in those with subdural hemorrhage and a CHA2DS2-VASc score of 0, to 33.3% in those with intracerebral hemorrhage and a CHA2DS2-VASc score of 9.
In a large, heterogeneous cohort, patients with atrial fibrillation faced a substantially heightened risk of ischemic stroke after intracranial hemorrhage. The risk was most marked in those with intracerebral hemorrhage and high CHA2DS2-VASc scores.
我们旨在评估心房颤动患者颅内出血后发生缺血性卒中的风险。
利用2005年至2012年加利福尼亚州、佛罗里达州和纽约州所有非联邦急症医院及急诊科的出院数据,我们确定了首次记录诊断为心房颤动时的患者。使用经过验证的诊断编码识别缺血性卒中和颅内出血。采用Kaplan-Meier生存统计和Cox比例风险分析来评估缺血性卒中的累积发生率以及颅内出血事件与随后卒中之间的关系。
在2,084,735例心房颤动患者中,50,468例(2.4%)发生颅内出血,89,594例(4.3%)在平均3.2年的随访期内发生缺血性卒中。脑出血后1年卒中累积发生率为8.1%(95%可信区间[CI],7.5 - 8.7%),硬膜下出血后为3.9%(95% CI,3.5 - 4.3%),无颅内出血者为2.0%(95% CI,2.0 - 2.1%)。在对CHA2DS2-VASc评分进行调整后,脑出血(风险比[HR],2.8;95% CI,2.6 - 2.9)和硬膜下出血(HR,1.6;95% CI,1.5 - 1.7)后卒中风险均升高。卒中的1年累积发生率范围从硬膜下出血且CHA2DS2-VASc评分为0者的0.9%,到脑出血且CHA2DS2-VASc评分为9者的33.3%。
在一个大型、异质性队列中,心房颤动患者颅内出血后发生缺血性卒中的风险显著升高。这种风险在脑出血且CHA2DS2-VASc评分高的患者中最为明显。