Miyata Yoshinori, Touyama Tetsuo, Kusumi Takaya, Morita Yoshitaka, Mizunuma Nobuyuki, Taniguchi Fumihiro, Manabe Mitsuaki
Department of Medical Oncology, Saku Central Hospital Advanced Care Center, 3400-28 Nakagomi, Saku, Nagano, 385-0051, Japan.
Department of Surgery, Nakagami Hospital, Okinawa, Japan.
Int J Clin Oncol. 2016 Aug;21(4):696-703. doi: 10.1007/s10147-015-0937-x. Epub 2015 Dec 28.
Irinotecan (CPT-11)-induced neutropenia is associated with UDP-glucuronosyltransferase (UGT) 1A1*6 and *28 polymorphisms. This prospective study investigated whether using these polymorphisms to adjust the initial dose of CPT-11 as part of FOLFIRI treatment in colorectal cancer patients might improve safety.
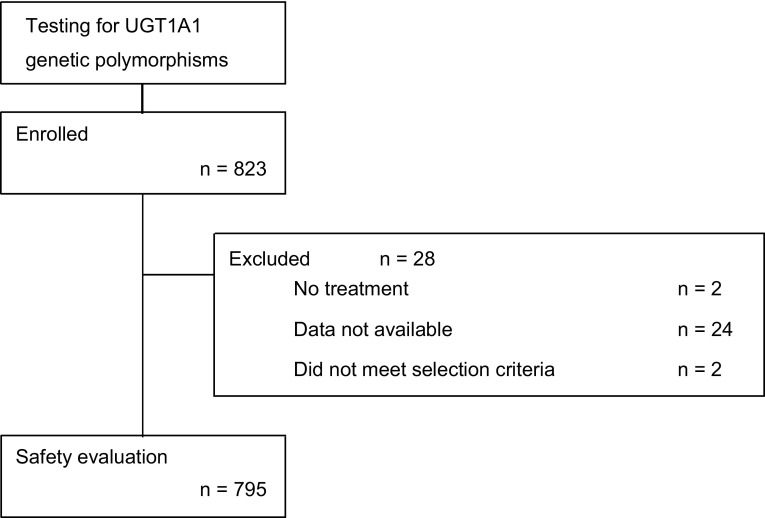
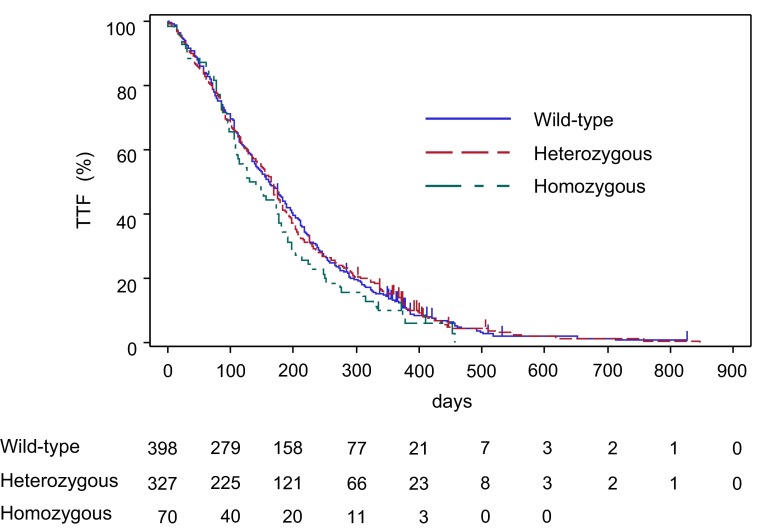
All data were collected by a physician. The relationship between UGT1A1 polymorphisms and first-cycle neutropenia, reasons for treatment discontinuation, and time-to-treatment failure were evaluated. Multivariate analysis was used to assess the risk of neutropenia.
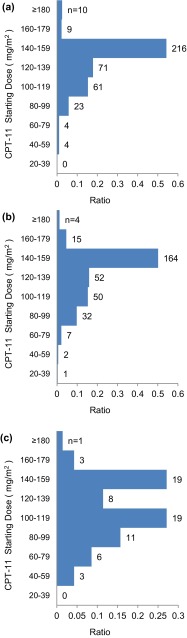
A total of 795 patients were divided into wild-type (*1/*1) (50.1 %), heterozygous (*28/*1, *6/*1) (41.1 %), and homozygous (*28/*28, *6/*6, *28/*6) (8.8 %) groups, in which the median starting dose of CPT-11 was 143.0, 143.0, and 115.0 mg/m(2), respectively. First-cycle grade ≥3 neutropenia occurred in 17.3, 25.4, and 28.6 % of these patients, respectively. Multivariate analysis revealed that the incidence of grade ≥3 neutropenia was significantly greater in the heterozygous and homozygous groups than in the wild-type group [odds ratio (OR) 1.67; 95 % confidence interval (CI) 1.16-2.42; p = 0.0060, and OR 2.22; 95 % CI 1.22-4.02; p = 0.0088, respectively]. Age (OR 1.77; 95 % CI 1.24-2.53; p = 0.0017), coelomic fluid (OR 1.84; 95 % CI 1.05-3.25; p = 0.0343), and non-reduction in starting dose (OR 1.53; 95 % CI 1.08-2.18; p = 0.0176) were also identified as significant risk factors.
The risk of neutropenia was higher in the heterozygous and homozygous groups at initiation of CPT-11 treatment. This suggests that when a reduction in dose is required in patients harboring two variant alleles, the decrease should be approximately 20 %.
伊立替康(CPT - 11)诱导的中性粒细胞减少与尿苷二磷酸葡萄糖醛酸基转移酶(UGT)1A16和28基因多态性相关。这项前瞻性研究调查了在结直肠癌患者中,将这些基因多态性用于调整CPT - 11的初始剂量作为FOLFIRI治疗的一部分是否可能提高安全性。
所有数据由一名医生收集。评估UGT1A1基因多态性与首个疗程中性粒细胞减少、治疗中断原因以及治疗失败时间之间的关系。采用多变量分析评估中性粒细胞减少的风险。
总共795例患者被分为野生型(*1/*1)(50.1%)、杂合子(*28/*1,*6/*1)(41.1%)和纯合子(*28/*28,*6/*6,*28/*6)(8.8%)组,其中CPT - 11的中位起始剂量分别为143.0、143.0和115.0mg/m²。这些患者中首个疗程≥3级中性粒细胞减少的发生率分别为17.3%、25.4%和28.6%。多变量分析显示,杂合子组和纯合子组≥3级中性粒细胞减少的发生率显著高于野生型组[比值比(OR)1.67;95%置信区间(CI)1.16 - 2.42;p = 0.0060,以及OR 2.22;95% CI 1.22 - 4.02;p = 0.0088]。年龄(OR 1.77;95% CI 1.24 - 2.53;p = 0.0017)、腹腔积液(OR 1.84;95% CI 1.05 - 3.25;p = 0.0343)和起始剂量未降低(OR 1.53;95% CI 1.08 - 2.18;p = 0.0176)也被确定为显著的风险因素。
CPT - 11治疗开始时,杂合子组和纯合子组中性粒细胞减少的风险较高。这表明在携带两个变异等位基因的患者中需要降低剂量时,减少幅度应约为20%。