Efsen Anne Marie W, Schultze Anna, Post Frank A, Panteleev Alexander, Furrer Hansjakob, Miller Robert F, Losso Marcelo H, Toibaro Javier, Skrahin Aliaksandr, Miro Jose M, Caylà Joan A, Girardi Enrico, Bruyand Mathias, Obel Niels, Podlekareva Daria N, Lundgren Jens D, Mocroft Amanda, Kirk Ole
Centre for Health and Infectious Disease Research (CHIP), Department of Infectious Diseases and Rheumatology, CHIP, Finsencentret, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
Department of Infection and Population Health, University College London Medical School, London, United Kingdom.
PLoS One. 2015 Dec 30;10(12):e0145380. doi: 10.1371/journal.pone.0145380. eCollection 2015.
Rates of TB/HIV coinfection and multi-drug resistant (MDR)-TB are increasing in Eastern Europe (EE). We aimed to study clinical characteristics, factors associated with MDR-TB and predicted activity of empiric anti-TB treatment at time of TB diagnosis among TB/HIV coinfected patients in EE, Western Europe (WE) and Latin America (LA).
Between January 1, 2011, and December 31, 2013, 1413 TB/HIV patients (62 clinics in 19 countries in EE, WE, Southern Europe (SE), and LA) were enrolled.
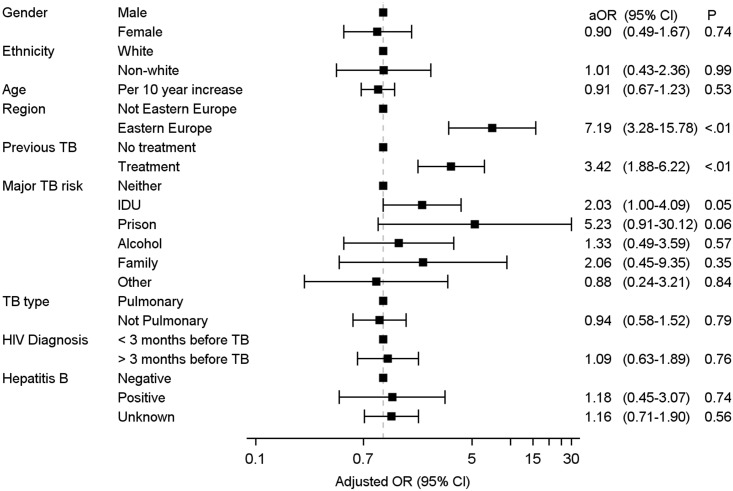
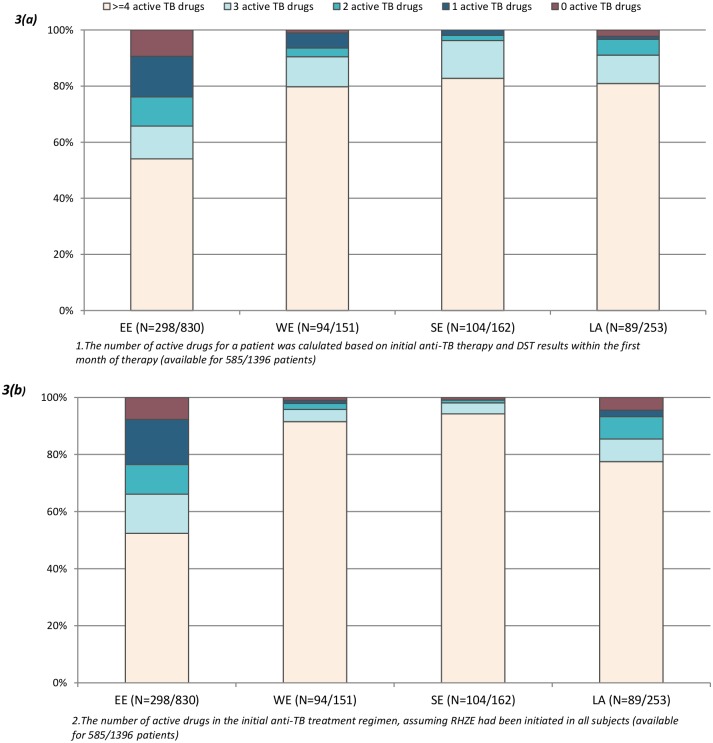
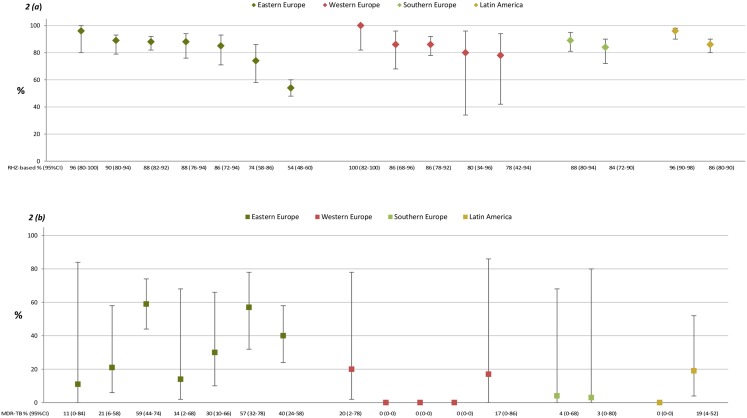
Significant differences were observed between EE (N = 844), WE (N = 152), SE (N = 164), and LA (N = 253) in the proportion of patients with a definite TB diagnosis (47%, 71%, 72% and 40%, p<0.0001), MDR-TB (40%, 5%, 3% and 15%, p<0.0001), and use of combination antiretroviral therapy (cART) (17%, 40%, 44% and 35%, p<0.0001). Injecting drug use (adjusted OR (aOR) = 2.03 (95% CI 1.00-4.09), prior anti-TB treatment (3.42 (1.88-6.22)), and living in EE (7.19 (3.28-15.78)) were associated with MDR-TB. Among 585 patients with drug susceptibility test (DST) results, the empiric (i.e. without knowledge of the DST results) anti-TB treatment included ≥3 active drugs in 66% of participants in EE compared with 90-96% in other regions (p<0.0001).
In EE, TB/HIV patients were less likely to receive a definite TB diagnosis, more likely to house MDR-TB and commonly received empiric anti-TB treatment with reduced activity. Improved management of TB/HIV patients in EE requires better access to TB diagnostics including DSTs, empiric anti-TB therapy directed at both susceptible and MDR-TB, and more widespread use of cART.
在东欧,结核病/艾滋病病毒合并感染率和耐多药结核病(MDR-TB)发病率不断上升。我们旨在研究东欧、西欧和拉丁美洲结核病/艾滋病病毒合并感染患者在结核病诊断时的临床特征、与耐多药结核病相关的因素以及经验性抗结核治疗的预测活性。
2011年1月1日至2013年12月31日期间,招募了1413例结核病/艾滋病病毒患者(来自东欧、西欧、南欧和拉丁美洲19个国家的62家诊所)。
在确诊结核病的患者比例(47%、71%、72%和40%,p<0.0001)、耐多药结核病(40%、5%、3%和15%,p<0.0001)以及联合抗逆转录病毒治疗(cART)的使用情况(17%、40%、44%和35%,p<0.0001)方面,东欧(N = 844)、西欧(N = 152)、南欧(N = 164)和拉丁美洲(N = 253)之间存在显著差异。注射吸毒(校正比值比(aOR)= 2.03(95%置信区间1.00 - 4.09))、既往抗结核治疗(3.42(1.88 - 6.22))以及居住在东欧(7.19(3.28 - 15.78))与耐多药结核病相关。在585例有药敏试验(DST)结果的患者中,经验性(即不知道DST结果)抗结核治疗在东欧66%的参与者中包括≥3种活性药物,而在其他地区为90 - 96%(p<0.0001)。
在东欧,结核病/艾滋病病毒患者确诊结核病的可能性较小,感染耐多药结核病的可能性较大,且通常接受活性较低的经验性抗结核治疗。改善东欧结核病/艾滋病病毒患者的管理需要更好地获得包括药敏试验在内的结核病诊断方法、针对敏感结核病和耐多药结核病的经验性抗结核治疗,以及更广泛地使用cART。