Mendes Pedro Vitale, Park Marcelo, Maciel Alexandre Toledo, E Silva Débora Prudêncio, Friedrich Natalia, Barbosa Edzangela Vasconcelos Santos, Hirota Adriana Sayuri, Schettino Guilherme Pinto Paula, Azevedo Luciano Cesar Pontes, Costa Eduardo Leite Vieira
Research and Education Institute, Hospital Sírio-Libanês, São Paulo, Brazil.
Intensive Care Unit, Hospital das Clinicas, University of São Paulo School of Medicine, Sixth floor-room 6040, Rua Dr. Eneas Carvalho de Aguiar, 255, São Paulo, 05623-010, Brazil.
Intensive Care Med Exp. 2016 Dec;4(1):1. doi: 10.1186/s40635-015-0074-x. Epub 2016 Jan 6.
Extracorporeal membrane oxygenation (ECMO) is a technique widely used worldwide to improve gas exchange. Changes in ECMO settings affect both oxygen and carbon dioxide. The impact on oxygenation can be followed closely by continuous pulse oximeter. Conversely, carbon dioxide equilibrates much slower and is not usually monitored directly.
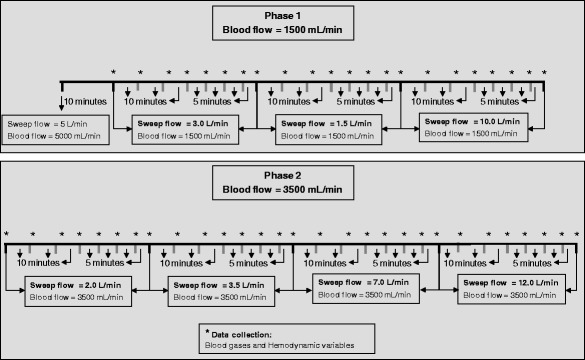
We investigated the time to stabilization of arterial carbon dioxide partial pressure (PaCO2) following step changes in ECMO settings in 5 apnoeic porcine models under veno-venous ECMO support with polymethylpentene membranes. We collected sequential arterial blood gases at a pre-specified interval of 50 min using a sequence of standardized blood and sweep gas flow combinations.
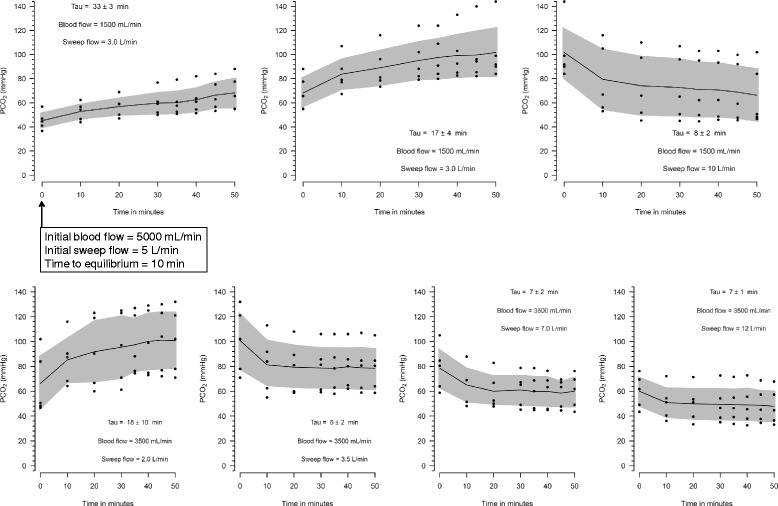
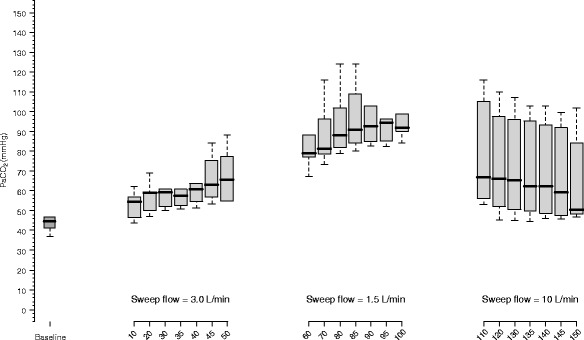
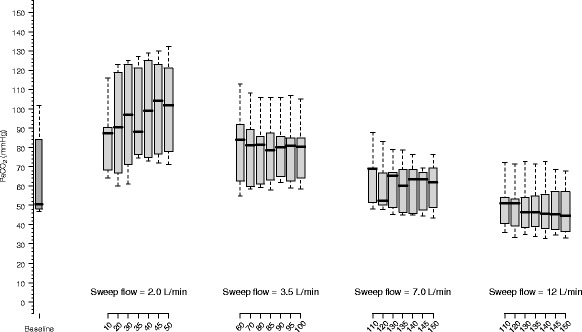
Following the changes in ECMO parameters, the kinetics of carbon dioxide was dependent on sweep gas and ECMO blood flow. With a blood flow of 1500 mL/min, PaCO2 takes longer than 50 min to equilibrate following the changes in sweep gas flow. Furthermore, the sweep gas flow from 3.0 to 10.0 L/min did not significantly affect PaCO2. However, with a blood flow of 3500 mL/min, 50 min was enough for PaCO2 to reach the equilibrium and every increment of sweep gas flow (up to 10.0 L/min) resulted in additional reductions of PaCO2.
Fifty minutes was enough to reach the equilibrium of PaCO2 after ECMO initiation or after changes in blood and sweep gas flow with an ECMO blood flow of 3500 ml/min. Longer periods may be necessary with lower ECMO blood flows.
体外膜肺氧合(ECMO)是一种在全球广泛应用以改善气体交换的技术。ECMO设置的改变会影响氧气和二氧化碳。连续脉搏血氧仪可密切监测对氧合的影响。相反,二氧化碳平衡要慢得多,通常不直接进行监测。
我们在5个采用聚甲基戊烯膜的静脉 - 静脉ECMO支持下的呼吸暂停猪模型中,研究了ECMO设置发生阶跃变化后动脉二氧化碳分压(PaCO2)达到稳定所需的时间。我们使用一系列标准化的血液和吹扫气体流量组合,以预先设定的50分钟间隔采集连续的动脉血气样本。
在ECMO参数改变后,二氧化碳的动力学取决于吹扫气体和ECMO血流量。当血流量为1500毫升/分钟时,吹扫气体流量改变后,PaCO2达到平衡所需时间超过50分钟。此外,吹扫气体流量从3.0升至10.0升/分钟对PaCO2没有显著影响。然而,当血流量为3500毫升/分钟时,50分钟足以使PaCO2达到平衡,并且吹扫气体流量每增加一次(直至10.0升/分钟)都会使PaCO2进一步降低。
对于血流量为3500毫升/分钟的ECMO,启动后或血液及吹扫气体流量改变后,50分钟足以使PaCO2达到平衡。ECMO血流量较低时可能需要更长时间。