Sood Neeraj, Wagner Zachary
Sol Price School of Public Policy and School of Pharmacy, University of Southern California, Los Angeles, California, USA Leonard D. Schaeffer Center for Health Policy and Economics, University of Southern California, Los Angeles, California, USA National Bureau of Economic Research, Cambridge, Massachusetts, USA.
School of Public Health, University of California Berkeley, Berkeley, California, USA.
BMJ Open. 2016 Jan 6;6(1):e010512. doi: 10.1136/bmjopen-2015-010512.
To evaluate the effects of a government insurance programme covering tertiary care for the poor in Karnataka, India--Vajpayee Arogyashree Scheme (VAS)--on treatment seeking and postoperative outcomes.
Geographic regression discontinuity.
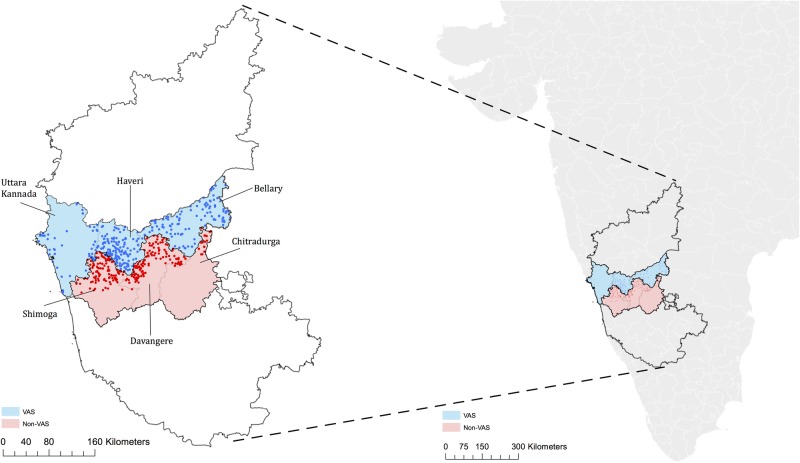
572 villages in Karnataka, India.
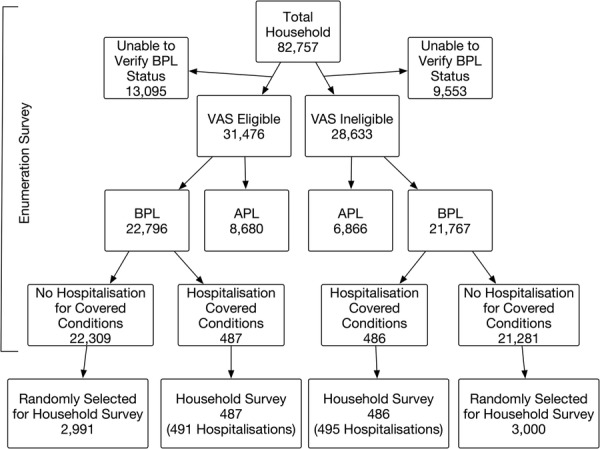
3478 households in 300 villages where VAS was implemented and 3486 households in 272 neighbouring matched villages ineligible for VAS.
A government insurance programme that provided free tertiary care to households below the poverty line in half of villages in Karnataka from February 2010 to August 2012.
Seeking treatment for symptoms, posthospitalisation well-being, occurrence of infections during hospitalisation and need for rehospitalisation.
The prevalence of symptoms was nearly identical for households in VAS-eligible villages compared with households in VAS-ineligible villages. However, households eligible for VAS were 4.96 percentage points (95% CI 1 to 8.9; p=0.014) more likely to seek treatment for their symptoms. The increase in treatment seeking was more pronounced for symptoms of cardiac conditions, the condition most frequently covered by VAS. Respondents from VAS-eligible villages reported greater improvements in well-being after a hospitalisation in all categories assessed and they were statistically significant in 3 of the 6 categories (walking ability, pain and anxiety). Respondents eligible for VAS were 9.4 percentage points less likely to report any infection after their hospitalisation (95% CI -20.2 to 1.4; p=0.087) and 16.5 percentage points less likely to have to be rehospitalised after the initial hospitalisation (95% CI -28.7 to -4.3; p<0.01).
Insurance for tertiary care increased treatment seeking among eligible households. Moreover, insured patients experienced better posthospitalisation outcomes, suggesting better quality of care received. These results suggest that there are several pathways through which tertiary care insurance could improve health, aside from increasing utilisation of the services that the programme directly subsidises.
评估印度卡纳塔克邦一项为贫困人口提供三级医疗保障的政府保险计划——瓦杰帕伊阿罗吉亚什里计划(VAS)——对就医行为和术后结果的影响。
地理回归间断性研究。
印度卡纳塔克邦的572个村庄。
在实施VAS的300个村庄中的3478户家庭,以及在272个相邻且不符合VAS资格的匹配村庄中的3486户家庭。
一项政府保险计划,从2010年2月至2012年8月为卡纳塔克邦一半村庄中生活在贫困线以下的家庭提供免费三级医疗服务。
因症状就医情况、住院后健康状况、住院期间感染发生率以及再次住院需求。
符合VAS资格村庄的家庭与不符合VAS资格村庄的家庭相比,症状发生率几乎相同。然而,符合VAS资格的家庭因症状寻求治疗的可能性高出4.96个百分点(95%置信区间为1至8.9;p=0.014)。对于心脏病症状(VAS最常涵盖的病症),寻求治疗的增加更为明显。来自符合VAS资格村庄的受访者在所有评估类别中均报告住院后健康状况有更大改善,且在6个类别中的3个类别(行走能力、疼痛和焦虑)具有统计学意义。符合VAS资格的受访者住院后报告有任何感染的可能性低9.4个百分点(95%置信区间为-20.2至1.4;p=0.087),初次住院后再次住院的可能性低16.5个百分点(95%置信区间为-28.7至-4.3;p<0.01)。
三级医疗保障保险增加了符合资格家庭的就医行为。此外,参保患者住院后的结果更好,表明获得了更高质量的医疗服务。这些结果表明,除了增加对该计划直接补贴的服务的利用外,三级医疗保障保险还可以通过多种途径改善健康状况。