Qin Vicky Mengqi, Hone Thomas, Millett Christopher, Moreno-Serra Rodrigo, McPake Barbara, Atun Rifat, Lee John Tayu
Saw Swee Hock School of Public Health, National University of Singapore, Singapore, Singapore.
Public Health Policy Evaluation Unit, Department of Primary Care and Public Health, School of Public Health, Imperial College, London, UK.
BMJ Glob Health. 2019 Jan 10;3(Suppl 3):e001087. doi: 10.1136/bmjgh-2018-001087. eCollection 2018.
User charges are widely used health financing mechanisms in many health systems in low-income and middle-income countries (LMICs) due to insufficient public health spending on health. This study systematically reviews the evidence on the relationship between user charges and health outcomes in LMICs, and explores underlying mechanisms of this relationship.
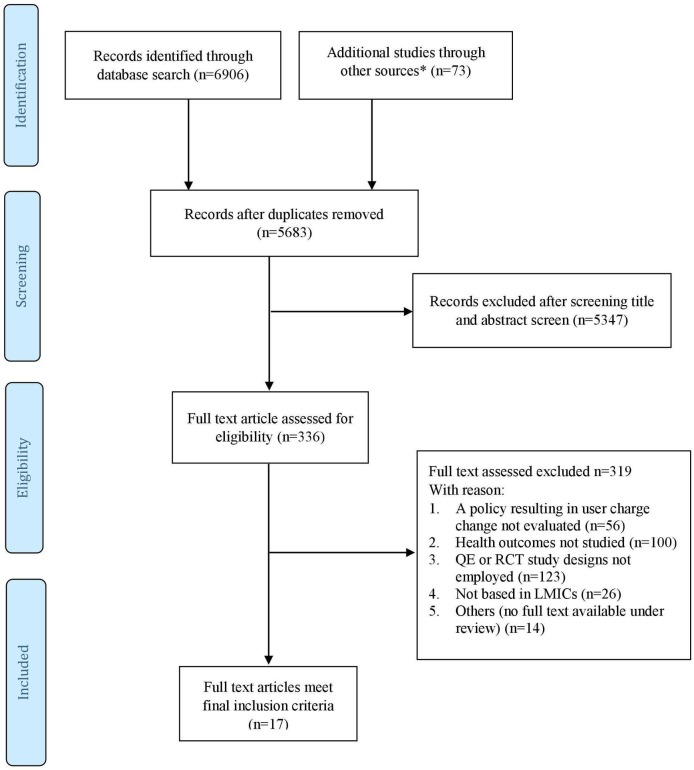
Published studies were identified via electronic medical, public health, health services and economics databases from 1990 to September 2017. We included studies that evaluated the impact of user charges on health in LMICs using randomised control trial (RCT) or quasi-experimental (QE) study designs. Study quality was assessed using Cochrane Risk of Bias and Risk of Bias in Non-Randomized Studies-of Intervention for RCT and QE studies, respectively.
We identified 17 studies from 12 countries (five upper-middle income countries, five lower-middle income countries and two low-income countries) that met our selection criteria. The findings suggested a modest relationship between reduction in user charges and improvements in health outcomes, but this depended on health outcomes measured, the populations studied, study quality and policy settings. The relationship between reduced user charges and improved health outcomes was more evident in studies focusing on children and lower-income populations. Studies examining infectious disease-related outcomes, chronic disease management and nutritional outcomes were too few to draw meaningful conclusions. Improved access to healthcare as a result of reduction in out-of-pocket expenditure was identified as the possible causal pathway for improved health.
Reduced user charges were associated with improved health outcomes, particularly for lower-income groups and children in LMICs. Accelerating progress towards universal health coverage through prepayment mechanisms such as taxation and insurance can lead to improved health outcomes and reduced health inequalities in LMICs.
CRD 42017054737.
由于低收入和中等收入国家(LMICs)公共卫生支出不足,使用者付费是许多卫生系统中广泛采用的卫生筹资机制。本研究系统评价了LMICs中使用者付费与健康结果之间关系的证据,并探讨了这种关系的潜在机制。
通过电子医学、公共卫生、卫生服务和经济学数据库检索1990年至2017年9月发表的研究。我们纳入了使用随机对照试验(RCT)或准实验(QE)研究设计评估使用者付费对LMICs健康影响的研究。分别使用Cochrane偏倚风险和非随机干预研究中的偏倚风险评估RCT和QE研究的研究质量。
我们从12个国家(5个中高收入国家、5个中低收入国家和2个低收入国家)中识别出17项符合我们选择标准的研究。研究结果表明,降低使用者付费与改善健康结果之间存在适度的关系,但这取决于所测量的健康结果、所研究的人群、研究质量和政策背景。在关注儿童和低收入人群的研究中,降低使用者付费与改善健康结果之间的关系更为明显。研究传染病相关结果、慢性病管理和营养结果的研究太少,无法得出有意义的结论。因自付费用减少而改善了获得医疗服务的机会被确定为健康改善的可能因果途径。
降低使用者付费与改善健康结果相关,特别是对于LMICs中的低收入群体和儿童。通过税收和保险等预付机制加速实现全民健康覆盖的进程,可以改善LMICs的健康结果并减少健康不平等。
CRD 42017054737。