The George Institute for Global Health, New Delhi, India.
Faculty of Medicine, University of New South Wales, Sydney, Australia.
Int J Equity Health. 2023 Sep 27;22(1):197. doi: 10.1186/s12939-023-02005-2.
Increasing financial risk protection is a key feature of Universal Health Coverage and the path towards health for all. Publicly Funded Health Insurance Schemes (PFHIS) have been considered as one of the pathways to safeguard against financial shocks and potentially reduce Out-of-Pocket Expenditure (OOPE). The south Indian state of Kerala has roughly a decade-long experience in implementing PFHIS. To date, there have been very few assessments of the coverage of these schemes and their impact on expenditure. Aiming to fill this gap, we explored the extent of and inequalities in insurance coverage, as well as choice of providers, and median cost of hospitalization in Kerala among insured and uninsured individuals.
A cross-sectional household survey was conducted in four districts of Kerala as part of a larger health systems research study from July-October 2019. We employed multistage random sampling to collect data from 13,064 individuals covering 3234 households in the catchment area of eight primary health care facilities. We used descriptive statistics, bivariate and multivariate analysis. We evaluated socioeconomic disparities using an absolute measure of inequality-the Slope Index of Inequality (SII) and a relative measure-the Relative Concentration Index (RCI).
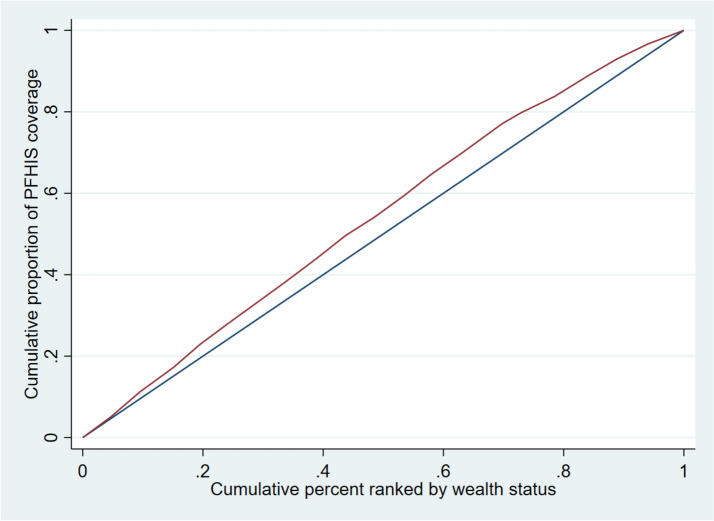
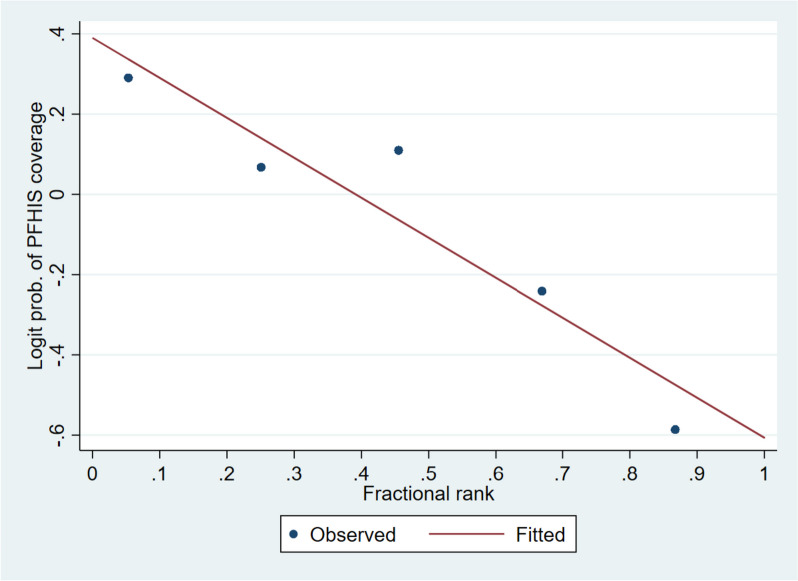
A substantial proportion of our study respondents reported that they were covered by PFHIS (45.8%). Respondents belonging to lowest and middle wealth quintiles of household had significantly greater odds of being covered by insurance than respondents belonging to the richest wealth quintile. The negative magnitude of RCI [-16.8% (95%CI: -25.3, -8.4)] and SII [-21.5% (95%CI: -36.1, -7.0)] suggest a higher concentration of PFHIS coverage among the poor. Median OOPE for hospitalisation at private health facilities was INR 9000 (approx. USD 108.70) among those covered by PFHIS, whereas it was INR 10500 (approx. USD 126.82) at private health facilities among those not covered by insurance.
While PFHIS seems to be appropriately targeting poorer populations, among the insured, OOPE for hospitalization persists. Among the uninsured, population subgroups with advantage are spending the greatest amount, raising questions about whether those facing relative disadvantage are forgoing care altogether or seeking care using cheaper, public avenues. Further policy action to more effectively reduce financial burden among left behind eligible populations under PFHIS will be essential to UHC progress in the state.
增加财务风险保护是全民健康覆盖的一个关键特征,也是实现全民健康的途径。公共资助的健康保险计划(PFHIS)被认为是防范财务冲击和潜在减少自付支出(OOPE)的途径之一。印度南部的喀拉拉邦在实施 PFHIS 方面已有大约十年的经验。迄今为止,很少有评估这些计划的覆盖范围及其对支出影响的评估。为了填补这一空白,我们探讨了喀拉拉邦参保和未参保个人的保险覆盖范围及其不平等程度,以及选择提供者和住院中位数费用。
作为一项更大的卫生系统研究的一部分,我们于 2019 年 7 月至 10 月在喀拉拉邦的四个地区进行了一项横断面家庭调查。我们采用多阶段随机抽样方法,从 8 个初级保健设施的集水区中收集了覆盖 3234 户家庭的 13064 名个人的数据。我们使用描述性统计、双变量和多变量分析。我们使用绝对不平等衡量指标——斜率指数不平等(SII)和相对衡量指标——相对集中指数(RCI)评估社会经济差距。
我们的研究受访者中有相当一部分报告说他们参加了 PFHIS(45.8%)。与最富有财富五分位数的受访者相比,属于最低和中等财富五分位数的受访者更有可能参加保险。RCI 的负数值[-16.8%(95%CI:-25.3,-8.4)]和 SII [-21.5%(95%CI:-36.1,-7.0)]表明,PFHIS 覆盖范围在贫困人口中更为集中。在参加 PFHIS 的人中,在私立医疗机构住院的 OOPE 中位数为 INR9000(约合 108.70 美元),而在未参保的人中,在私立医疗机构住院的 OOPE 中位数为 INR10500(约合 126.82 美元)。
虽然 PFHIS 似乎适当地针对较贫穷的人群,但在参保人群中,住院的 OOPE 仍然存在。在未参保人群中,具有优势的人口亚群支出最多,这引发了一个问题,即那些面临相对劣势的人是否完全放弃了医疗服务,还是通过更便宜的公共途径寻求医疗服务。为了在该州的全民健康覆盖方面取得进一步进展,需要采取进一步的政策行动,以使 PFHIS 下遗留的符合条件的人群更有效地减轻经济负担。