Thongprayoon Charat, Cheungpasitporn Wisit, Harrison Andrew M, Kittanamongkolchai Wonngarm, Ungprasert Patompong, Srivali Narat, Akhoundi Abbasali, Kashani Kianoush B
Division of Nephrology and Hypertension, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Medical Scientist Training Program, Mayo Clinic, Rochester, MN, USA.
BMC Nephrol. 2016 Jan 9;17:6. doi: 10.1186/s12882-016-0220-z.
Baseline serum creatinine (SCr) level is frequently not measured in clinical practice. The aim of this study was to investigate the effect of various methods of baseline SCr determination measurement on accuracy of acute kidney injury (AKI) diagnosis in critically ill patients.
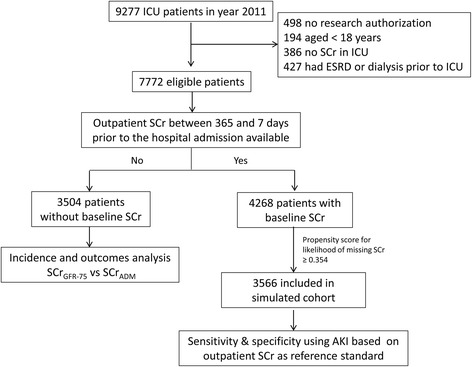
This was a retrospective cohort study. All adult intensive care unit (ICU) patients admitted at a tertiary referral hospital from January 1, 2011 through December 31, 2011, with at least one measured SCr value during ICU stay, were included in this study. The baseline SCr was considered either an admission SCr (SCrADM) or an estimated SCr, using MDRD formula, based on an assumed glomerular filtration rate (GFR) of 75 ml/min/1.73 m(2) (SCrGFR-75). Determination of AKI was based on the KDIGO SCr criterion. Propensity score to predict the likelihood of missing SCr was used to generate a simulated cohort of 3566 patients with baseline outpatient SCr, who had similar characteristics with patients whose outpatient SCr was not available.
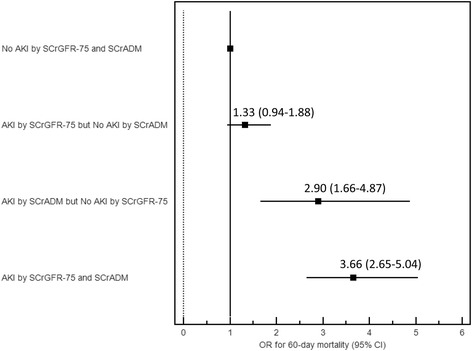
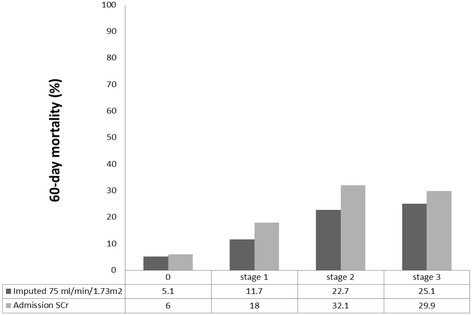
Of 7772 patients, 3504 (45.1 %) did not have baseline outpatient SCr. Among patients without baseline outpatient SCr, AKI was detected in 571 (16.3 %) using the SCrADM and 997 (28.4 %) using SCrGFR-75 (p < .001). Compared with non-AKI patients, patients who met AKI only by SCrADM, but not SCrGFR-75, were significantly associated with 60-day mortality (OR 2.90; 95 % CI 1.66-4.87), whereas patients who met AKI only by SCrGFR-75, but not SCrADM, had a non-significant increase in 60-day mortality risk (OR 1.33; 95 % CI 0.94-1.88). In a simulated cohort of patients with baseline outpatient SCr, SCrGFR-75 yielded a higher sensitivity (77.2 vs. 50.5 %) and lower specificity (87.8 vs. 94.8 %) for the AKI diagnosis in comparison with SCrADM.
When baseline outpatient SCr was not available, using SCrGFR-75 as surrogate for baseline SCr was found to be more sensitive but less specific for AKI diagnosis compared with using SCrADM. This resulted in higher incidence of AKI with larger likelihood of false-positive cases.
临床实践中常常不检测基线血清肌酐(SCr)水平。本研究的目的是探讨各种基线SCr测定方法对危重症患者急性肾损伤(AKI)诊断准确性的影响。
这是一项回顾性队列研究。纳入2011年1月1日至2011年12月31日在一家三级转诊医院收治的所有成年重症监护病房(ICU)患者,这些患者在ICU住院期间至少有一次SCr测量值。基线SCr被视为入院时的SCr(SCrADM)或根据假设的肾小球滤过率(GFR)为75 ml/min/1.73 m²使用MDRD公式估算的SCr(SCrGFR-75)。AKI的判定基于KDIGO的SCr标准。使用预测缺失SCr可能性的倾向评分来生成一个模拟队列,该队列包含3566例有门诊基线SCr的患者,其特征与无门诊SCr的患者相似。
在7772例患者中,3504例(45.1%)没有门诊基线SCr。在没有门诊基线SCr的患者中,使用SCrADM检测到AKI的有571例(16.3%),使用SCrGFR-75检测到AKI的有997例(28.4%)(p<0.001)。与非AKI患者相比,仅通过SCrADM符合AKI标准但未通过SCrGFR-75符合标准者,60天死亡率显著升高(OR 2.90;95%CI 1.66-4.87),而仅通过SCrGFR-75符合AKI标准但未通过SCrADM符合标准者,60天死亡风险虽有升高但无统计学意义(OR 1.33;95%CI 0.94-1.88)。在有门诊基线SCr的模拟队列患者中,与SCrADM相比,SCrGFR-75对AKI诊断的敏感性更高(77.2%对50.5%),但特异性更低(87.8%对94.8%)。
当没有门诊基线SCr时,与使用SCrADM相比,使用SCrGFR-75作为基线SCr的替代指标对AKI诊断更敏感但特异性更低。这导致AKI发病率更高,假阳性病例的可能性更大。