Dumitriu Bogdan, Ito Sawa, Feng Xingmin, Stephens Nicole, Yunce Muharrem, Kajigaya Sachiko, Melenhorst Joseph J, Rios Olga, Scheinberg Priscila, Chinian Fariba, Keyvanfar Keyvan, Battiwalla Minoo, Wu Colin O, Maric Irina, Xi Liqiang, Raffeld Mark, Muranski Pawel, Townsley Danielle M, Young Neal S, Barrett Austin J, Scheinberg Phillip
Hematology Branch, National Heart, Lung, and Blood Institute, National Institutes for Health, Bethesda, MD, USA.
Office of Biostatistics Research, National Heart, Lung, and Blood Institute, National Institutes for Health, Bethesda, MD, USA.
Lancet Haematol. 2016 Jan;3(1):e22-9. doi: 10.1016/S2352-3026(15)00227-6. Epub 2015 Dec 17.
T-cell large granular lymphocytic leukaemia (T-LGL) is a lymphoproliferative disease that presents with immune-mediated cytopenias and is characterised by clonal expansion of cytotoxic CD3+ CD8+ lymphocytes. Use of methotrexate, ciclosporin, or cyclophosphamide as first therapy improves cytopenias in 50% of patients, but long-term use of these can lead to toxicity. We aimed to explore the activity and safety of alemtuzumab, an anti-CD52 monoclonal antibody, in patients with T-LGL.
We did this single-arm, phase 2 trial in consecutively enrolled adults with T-LGL referred to the National Institutes of Health in Bethesda, MD, USA. Alemtuzumab was given intravenously at 10 mg per day for 10 days. The primary endpoint was haematological response at 3 months after infusion. A complete response was defined as normalisation of all affected lineages, and a partial response was defined in neutropenic patients as 100% increase in the absolute neutrophil count to more than 5 × 10(8) cells per L, and in those with anaemia, as any increase in haemoglobin of 20 g/L or higher observed in at least two serial measurements 1 week apart and sustained for 1 month or longer without exogenous growth factors support or transfusions. Analysis was by intention to treat. We report results from the first stage of this Simon two-stage design trial; enrolment into the second stage is continuing. This study is registered with ClinicalTrials.gov, number NCT00345345.
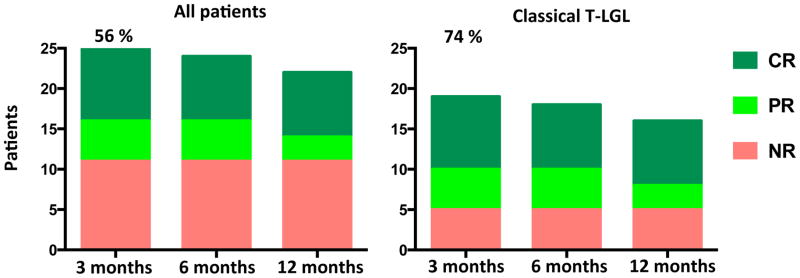
From Oct 1, 2006, to March 1, 2015, we enrolled 25 patients with T-LGL. 14 patients (56%; 95% CI 35-76) had a haematological response at 3 months. Four patients with associated myelodysplastic syndrome and two who had received haemopoietic stem cell transplantation had either no response or were not evaluable, meaning 14 (74% [49-91]) of the 19 patients with classic T-LGL responded. All patients had an infusion reaction (24 [96%] patients grade 1-2, one [4%] patient grade 3), which improved with symptomatic therapy. All patients developed lymphopenia, with 22 (88%) patients having grade 3 or 4 lymphopenia. The other most common grade 3 and 4 adverse events were leukopenia (eight [32%]) and neutropenic infections (five [20%]). Seven patients died; all were non-responders.
This is the largest and only prospective study of alemtuzumab in patients with T-LGL. The activity reported with a single course of a lymphocytotoxic drug in patients with mainly relapsed and refractory disease suggests that haematological response can be achieved without continued use of oral immunosuppression.
National Heart, Lung, and Blood Institute.
T 细胞大颗粒淋巴细胞白血病(T-LGL)是一种淋巴增殖性疾病,表现为免疫介导的血细胞减少,其特征是细胞毒性 CD3+CD8+淋巴细胞的克隆性扩增。使用甲氨蝶呤、环孢素或环磷酰胺作为一线治疗可使 50%的患者血细胞减少情况得到改善,但长期使用这些药物可能会导致毒性。我们旨在探讨抗 CD52 单克隆抗体阿仑单抗在 T-LGL 患者中的活性和安全性。
我们在美国马里兰州贝塞斯达的国立卫生研究院对连续入组的成年 T-LGL 患者进行了这项单臂 2 期试验。阿仑单抗静脉注射,每天 10 毫克,共 10 天。主要终点是输注后 3 个月的血液学反应。完全缓解定义为所有受累谱系恢复正常,部分缓解在中性粒细胞减少患者中定义为绝对中性粒细胞计数增加 100%,超过每升 5×10⁸个细胞,在贫血患者中定义为至少两次间隔 1 周的连续测量中血红蛋白增加 20 克/升或更高,并在无外源性生长因子支持或输血的情况下持续 1 个月或更长时间。分析采用意向性治疗。我们报告了这项西蒙两阶段设计试验第一阶段的结果;第二阶段的入组工作仍在继续。本研究已在 ClinicalTrials.gov 注册,编号为 NCT00345345。
从 2006 年 10 月 1 日至 2015 年 3 月 1 日,我们纳入了 25 例 T-LGL 患者。14 例患者(56%;95%CI 35 - 76)在 3 个月时有血液学反应。4 例合并骨髓增生异常综合征的患者和 2 例接受过造血干细胞移植的患者无反应或无法评估,这意味着 19 例经典 T-LGL 患者中有 14 例(74%[49 - 91])有反应。所有患者均出现输注反应(24 例[96%]患者为 1 - 2 级,1 例[4%]患者为 3 级),经对症治疗后有所改善。所有患者均出现淋巴细胞减少,22 例(88%)患者为 3 级或 4 级淋巴细胞减少。其他最常见的 3 级和 4 级不良事件为白细胞减少(8 例[32%])和中性粒细胞减少性感染(5 例[20%])。7 例患者死亡;均为无反应者。
这是关于阿仑单抗治疗 T-LGL 患者的规模最大且唯一的前瞻性研究。在主要为复发和难治性疾病的患者中使用一个疗程的淋巴细胞毒性药物所报告的活性表明,无需持续使用口服免疫抑制剂即可实现血液学反应。
美国国立心肺血液研究所。