Federici Lauren M, Caliman Izabela Facco, Molosh Andrei I, Fitz Stephanie D, Truitt William A, Bonaventure Pascal, Carpenter Janet S, Shekhar Anantha, Johnson Philip L
Department of Anatomy & Cell Biology, USA; Paul and Carole Stark Neurosciences Research Institute, USA; Program in Medical Neurosciences, Paul and Carole Stark Neurosciences Research Institute, USA.
Department of Anatomy & Cell Biology, USA; Paul and Carole Stark Neurosciences Research Institute, USA.
Psychoneuroendocrinology. 2016 Mar;65:127-37. doi: 10.1016/j.psyneuen.2015.12.011. Epub 2015 Dec 18.
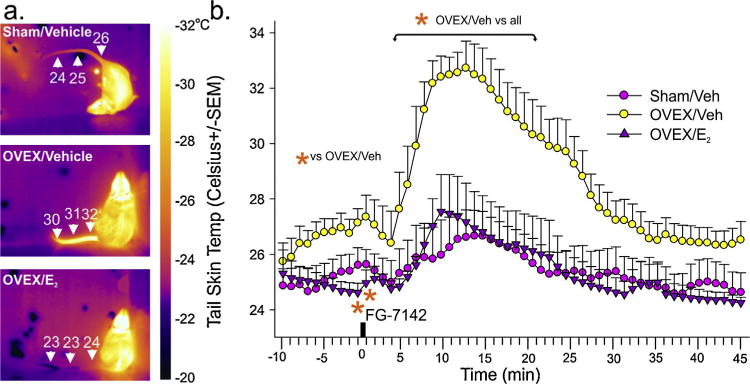
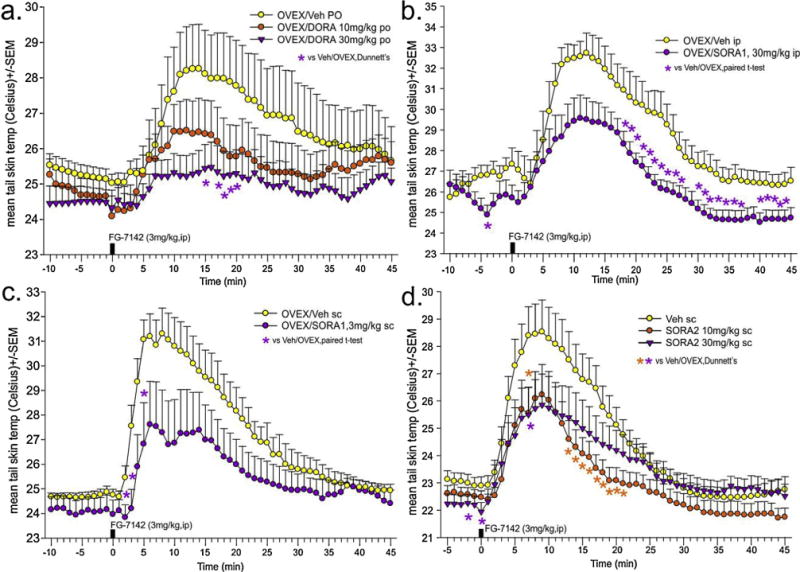
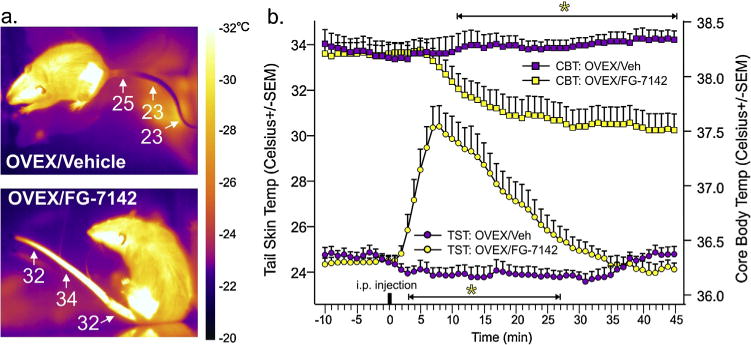
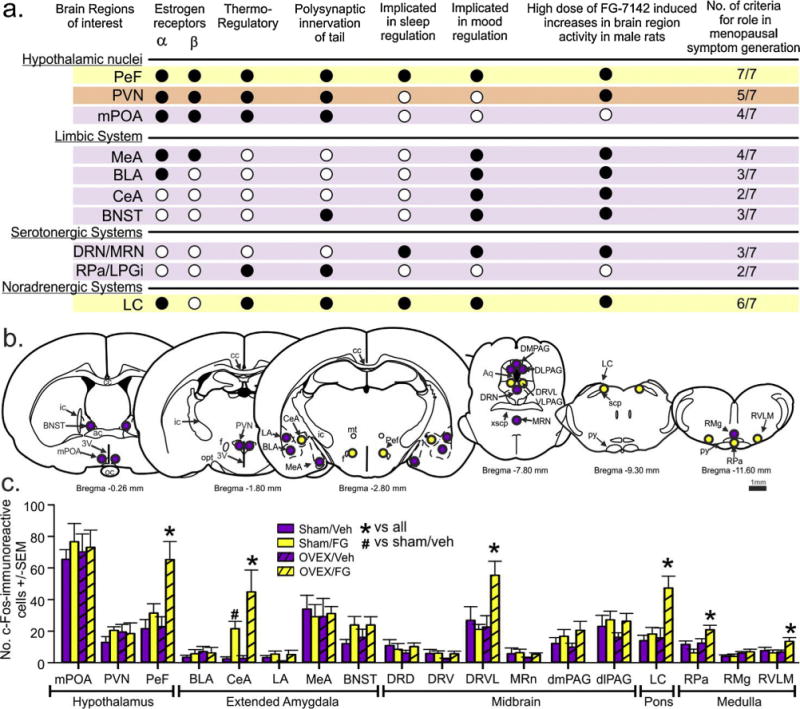
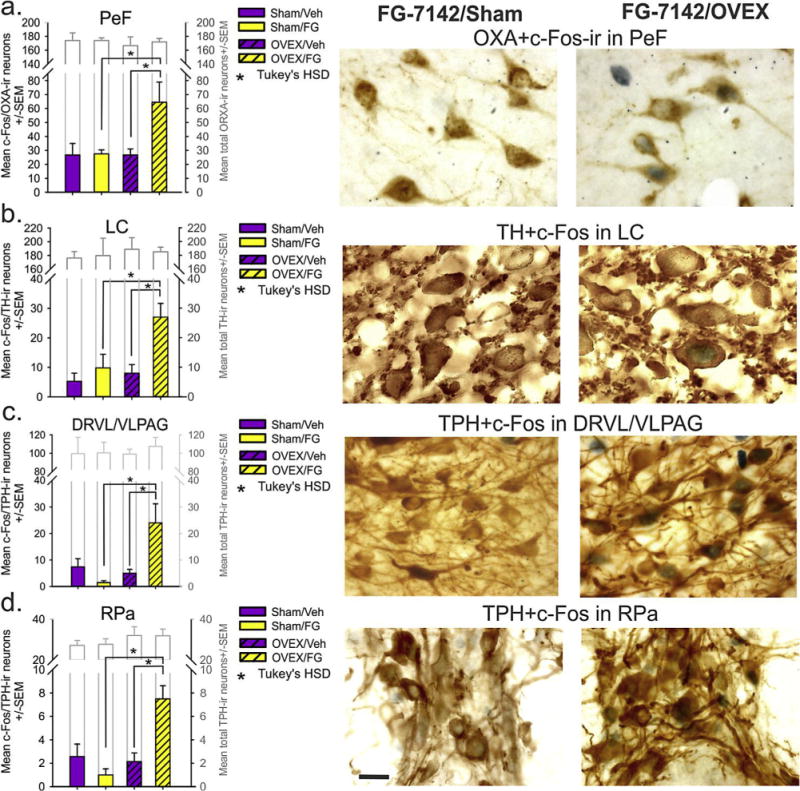
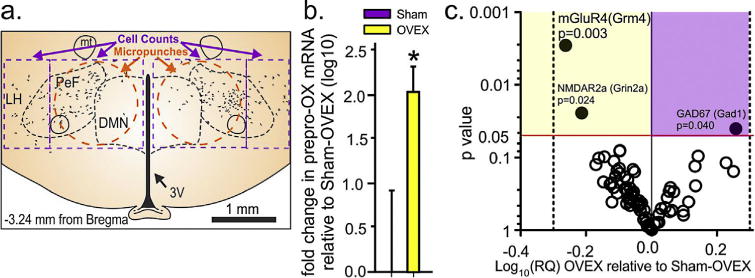
Distressing symptoms such as hot flashes and sleep disturbances affect over 70% of women approaching menopause for an average of 4-7 years, and recent large cohort studies have shown that anxiety and stress are strongly associated with more severe and persistent hot flashes and can induce hot flashes. Although high estrogen doses alleviate symptoms, extended use increases health risks, and current non-hormonal therapies are marginally better than placebo. The lack of effective non-hormonal treatments is largely due to the limited understanding of the mechanisms that underlie menopausal symptoms. One mechanistic pathway that has not been explored is the wake-promoting orexin neuropeptide system. Orexin is exclusively synthesized in the estrogen receptor rich perifornical hypothalamic region, and has an emerging role in anxiety and thermoregulation. In female rodents, estrogens tonically inhibit expression of orexin, and estrogen replacement normalizes severely elevated central orexin levels in postmenopausal women. Using an ovariectomy menopause model, we demonstrated that an anxiogenic compound elicited exacerbated hot flash-associated increases in tail skin temperature (TST, that is blocked with estrogen), and cellular responses in orexin neurons and efferent targets. Furthermore, systemic administration of centrally active, selective orexin 1 or 2 and dual receptor antagonists attenuated or blocked TST responses, respectively. This included the reformulated Suvorexant, which was recently FDA-approved for treating insomnia. Collectively, our data support the hypothesis that dramatic loss of estrogen tone during menopausal states leads to a hyperactive orexin system that contributes to symptoms such as anxiety, insomnia, and more severe hot flashes. Additionally, orexin receptor antagonists may represent a novel non-hormonal therapy for treating menopausal symptoms, with minimal side effects.
潮热和睡眠障碍等令人苦恼的症状影响超过70%的接近更年期的女性,平均持续4至7年,最近的大型队列研究表明,焦虑和压力与更严重、更持久的潮热密切相关,并且会诱发潮热。虽然高剂量雌激素可缓解症状,但长期使用会增加健康风险,而目前的非激素疗法仅略优于安慰剂。缺乏有效的非激素治疗方法很大程度上是由于对更年期症状背后的机制了解有限。一种尚未被探索的机制途径是促进觉醒的食欲素神经肽系统。食欲素仅在富含雌激素受体的下丘脑室周区域合成,并且在焦虑和体温调节中发挥着新出现的作用。在雌性啮齿动物中,雌激素可抑制食欲素的表达,而雌激素替代可使绝经后女性中枢食欲素水平严重升高恢复正常。使用卵巢切除更年期模型,我们证明一种致焦虑化合物会加剧与潮热相关的尾皮温度(TST)升高(这种升高可被雌激素阻断),以及食欲素神经元及其传出靶点的细胞反应。此外,全身给予中枢活性、选择性食欲素1或2以及双受体拮抗剂分别减弱或阻断了TST反应。这包括最近被美国食品药品监督管理局(FDA)批准用于治疗失眠的重新配方的苏沃雷生。总体而言,我们的数据支持这样一种假设,即更年期状态下雌激素水平的急剧下降会导致食欲素系统过度活跃,从而导致焦虑、失眠和更严重的潮热等症状。此外,食欲素受体拮抗剂可能代表一种治疗更年期症状的新型非激素疗法,副作用最小。