Bellolio M Fernanda, Gilani Waqas I, Barrionuevo Patricia, Murad M Hassan, Erwin Patricia J, Anderson Joel R, Miner James R, Hess Erik P
Department of Emergency Medicine, Mayo Clinic, Rochester, MN.
Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN.
Acad Emerg Med. 2016 Feb;23(2):119-34. doi: 10.1111/acem.12875. Epub 2016 Jan 22.
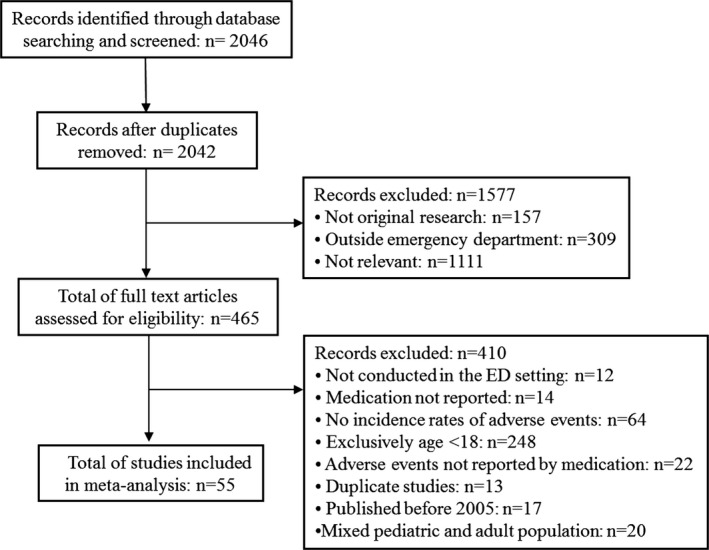
This was a systematic review and meta-analysis to evaluate the incidence of adverse events in adults undergoing procedural sedation in the emergency department (ED).
Eight electronic databases were searched, including MEDLINE, EMBASE, EBSCO, CINAHL, CENTRAL, Cochrane Database of Systematic Reviews, Web of Science, and Scopus, from January 2005 through 2015. Randomized controlled trials and observational studies of adults undergoing procedural sedation in the ED that reported a priori selected outcomes and adverse events were included. Meta-analysis was performed using a random-effects model and reported as incidence rates with 95% confidence intervals (CIs).
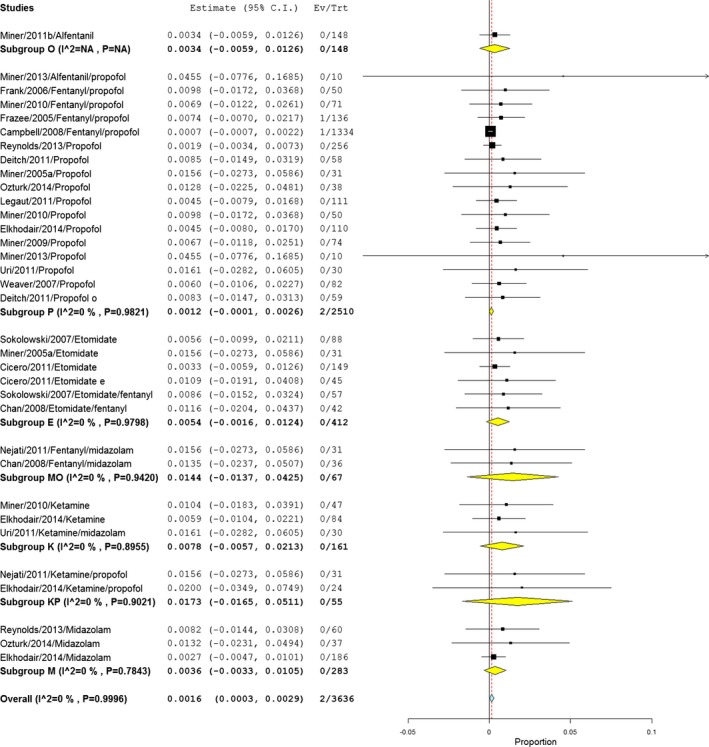
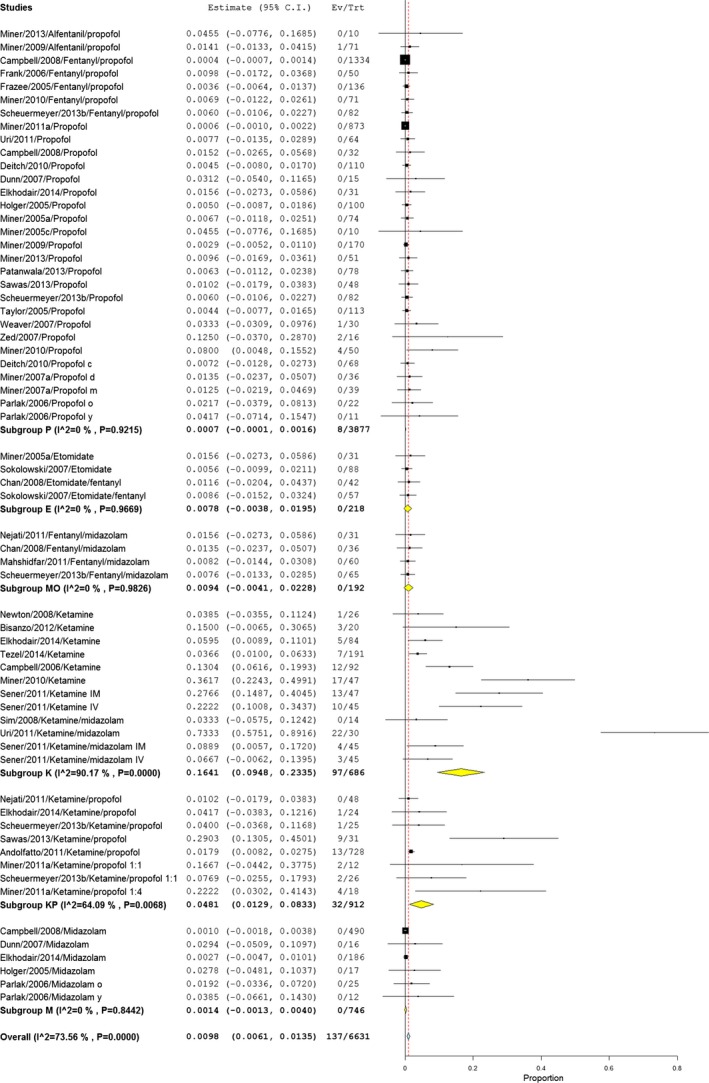
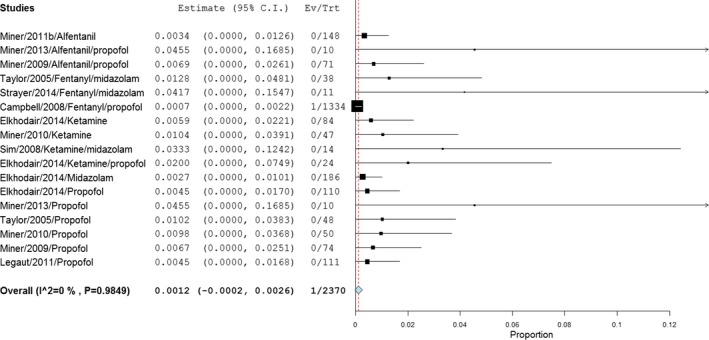
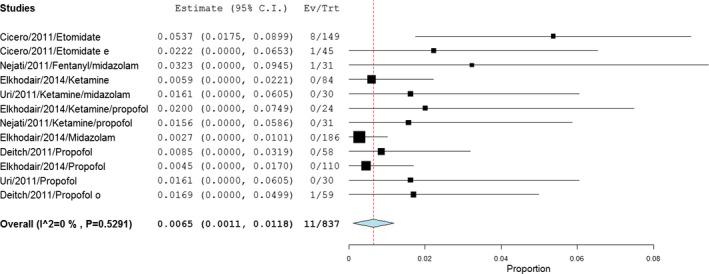
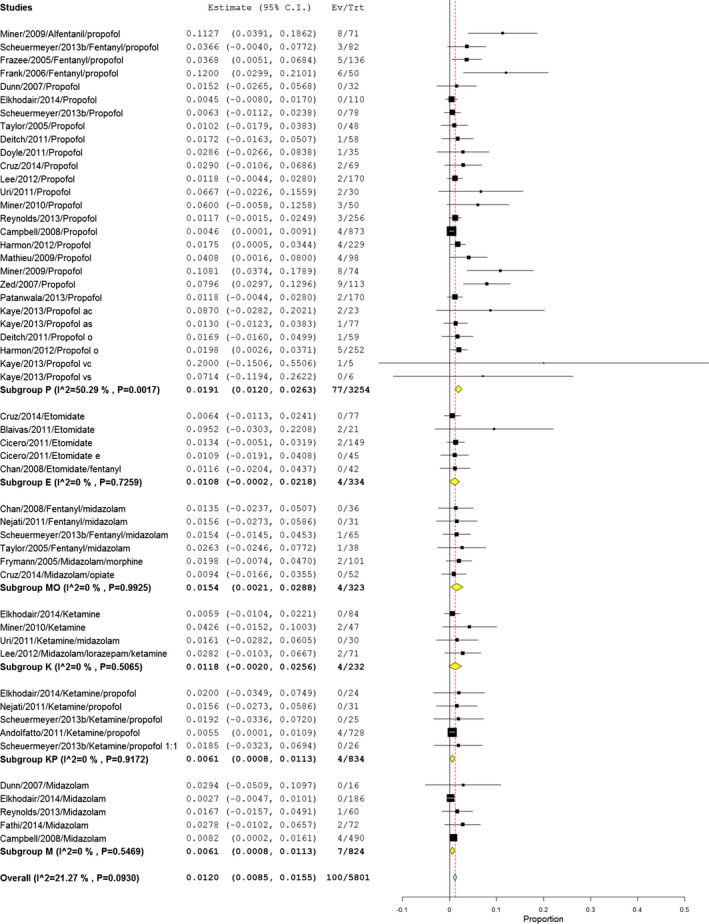
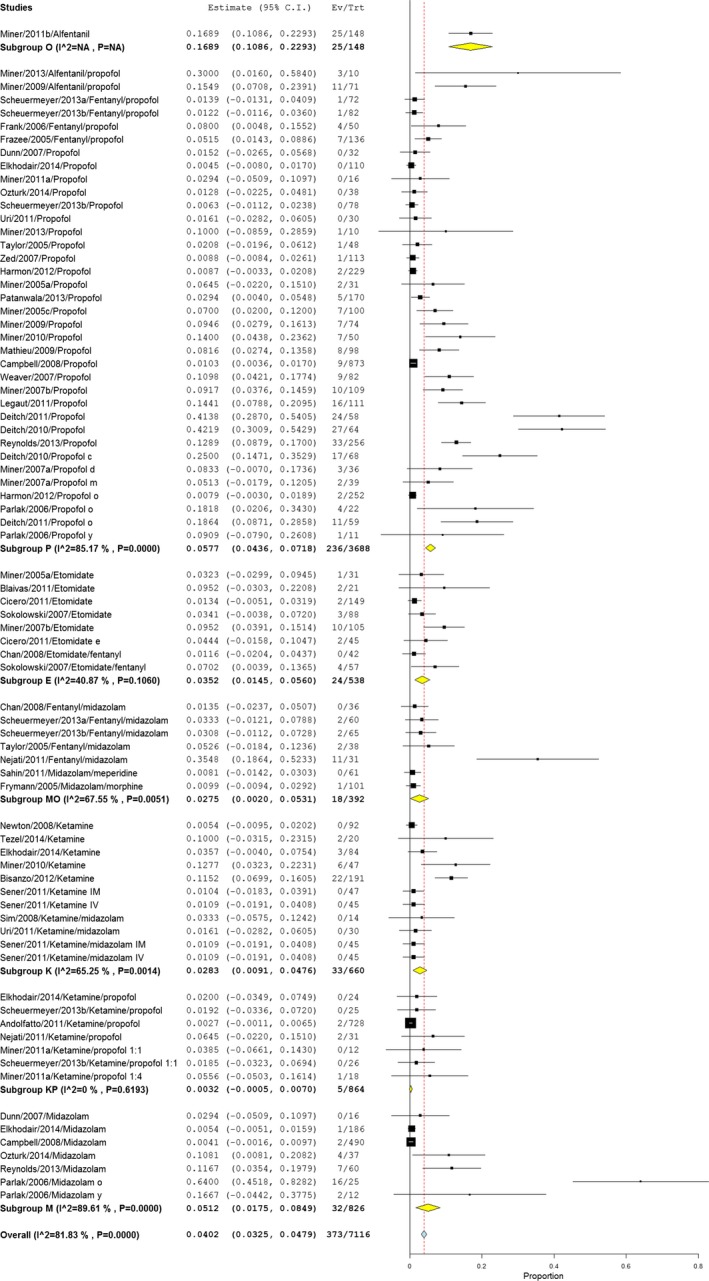
The search yielded 2,046 titles for review. Fifty-five articles were eligible, including 9,652 procedural sedations. The most common adverse event was hypoxia, with an incidence of 40.2 per 1,000 sedations (95% CI = 32.5 to 47.9), followed by vomiting with 16.4 per 1,000 sedations (95% CI = 9.7 to 23.0) and hypotension with 15.2 per 1,000 sedations (95% CI = 10.7 to 19.7). Severe adverse events requiring emergent medical intervention were rare, with one case of aspiration in 2,370 sedations (1.2 per 1,000), one case of laryngospasm in 883 sedations (4.2 per 1,000), and two intubations in 3,636 sedations (1.6 per 1,000). The incidence of agitation and vomiting were higher with ketamine (164.1 per 1,000 and 170.0 per 1,000, respectively). Apnea was more frequent with midazolam (51.4 per 1,000), and hypoxia was less frequent in patients who received ketamine/propofol compared to other combinations. The case of laryngospasm was in a patient who received ketamine, and the aspiration and intubations were in patients who received propofol. When propofol and ketamine are combined, the incidences of agitation, apnea, hypoxia, bradycardia, hypotension, and vomiting were lower compared to each medication separately.
Serious adverse events during procedural sedation like laryngospasm, aspiration, and intubation are exceedingly rare. Quantitative risk estimates are provided to facilitate shared decision-making, risk communication, and informed consent.
本研究为一项系统评价和荟萃分析,旨在评估急诊科接受程序性镇静的成人不良事件的发生率。
检索了8个电子数据库,包括MEDLINE、EMBASE、EBSCO、CINAHL、CENTRAL、Cochrane系统评价数据库、科学引文索引和Scopus,检索时间为2005年1月至2015年。纳入了关于急诊科接受程序性镇静的成人的随机对照试验和观察性研究,这些研究报告了预先选定的结局和不良事件。采用随机效应模型进行荟萃分析,并以95%置信区间(CI)的发生率报告结果。
检索共获得2046篇待审文献。55篇文章符合纳入标准,包括9652例程序性镇静。最常见的不良事件是低氧血症,发生率为每1000例镇静40.2例(95%CI=32.5至47.9),其次是呕吐,每1000例镇静16.4例(95%CI=9.7至23.0),低血压每1000例镇静15.2例(95%CI=10.7至19.7)。需要紧急医疗干预的严重不良事件很少见,2370例镇静中有1例误吸(每1000例1.2例),883例镇静中有1例喉痉挛(每1000例4.2例),3636例镇静中有2例插管(每1000例1.6例)。氯胺酮使用时躁动和呕吐的发生率较高(分别为每1000例164.1例和170.0例)。咪达唑仑使用时呼吸暂停更常见(每1000例51.4例),与其他联合用药相比,氯胺酮/丙泊酚联合使用的患者低氧血症发生率较低。喉痉挛的病例发生在接受氯胺酮治疗的患者中,误吸和插管的病例发生在接受丙泊酚治疗的患者中。丙泊酚和氯胺酮联合使用时,躁动、呼吸暂停、低氧血症、心动过缓、低血压和呕吐的发生率低于单独使用每种药物时。
程序性镇静期间如喉痉挛、误吸和插管等严重不良事件极为罕见。提供了定量风险估计值,以促进共同决策、风险沟通和知情同意。