Kimmoun Antoine, Baux Elisabeth, Das Vincent, Terzi Nicolas, Talec Patrice, Asfar Pierre, Ehrmann Stephan, Geri Guillaume, Grange Steven, Anguel Nadia, Demoule Alexandre, Moreau Anne Sophie, Azoulay Elie, Quenot Jean-Pierre, Boisramé-Helms Julie, Louis Guillaume, Sonneville Romain, Girerd Nicolas, Ducrocq Nicolas, Agrinier Nelly, Wahl Denis, Puéchal Xavier, Levy Bruno
Brabois Medical Intensive Care Unit, Nancy University Hospital, Vandoeuvre-les-Nancy, Nancy, 54000, France.
INSERM U1116, Vandoeuvre-les-Nancy, Nancy, France.
Crit Care. 2016 Jan 26;20:27. doi: 10.1186/s13054-016-1189-5.
The outcomes of patients admitted to the intensive care unit (ICU) for acute manifestation of small-vessel vasculitis are poorly reported. The aim of the present study was to determine the mortality rate and prognostic factors of patients admitted to the ICU for acute small-vessel vasculitis.
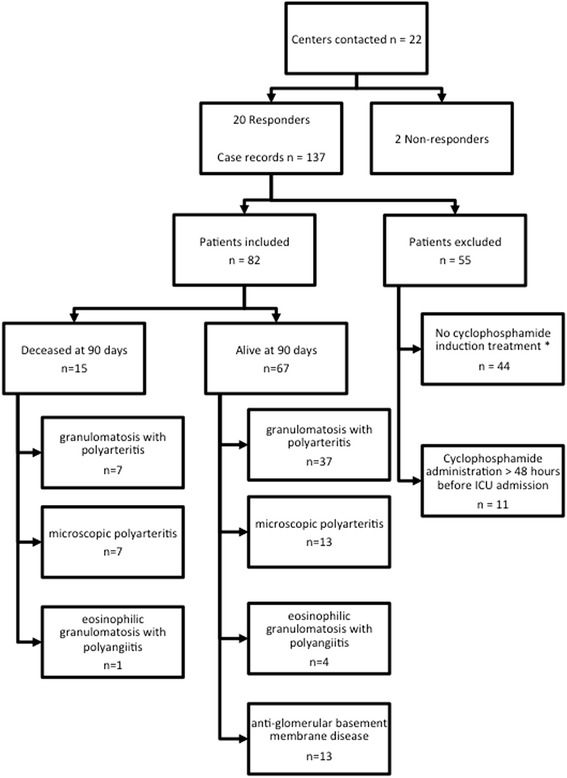
This retrospective, multicenter study was conducted from January 2001 to December 2014 in 20 ICUs in France. Patients were identified from computerized registers of each hospital using the International Classification of Diseases, Ninth Revision (ICD-9). Inclusion criteria were (1) known or highly suspected granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, microscopic polyangiitis (respectively, ICD-9 codes M31.3, M30.1, and M31.7), or anti-glomerular basement membrane antibody disease (ICD-9 codes N08.5X-005 or M31.0+); (2) admission to the ICU for the management of an acute manifestation of vasculitis; and (3) administration of a cyclophosphamide pulse in the ICU or within 48 h before admission to the ICU. The primary endpoint was assessment of mortality rate 90 days after admission to the ICU.
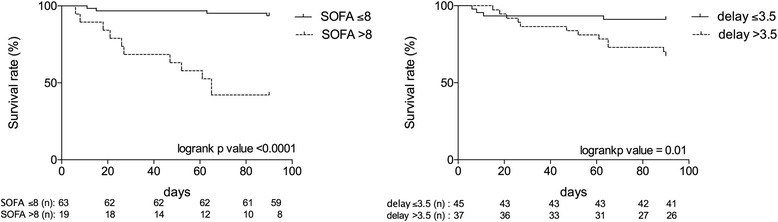
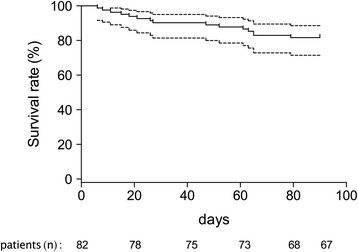
Eighty-two patients at 20 centers were included, 94% of whom had a recent (<6 months) diagnosis of small-vessel vasculitis. Forty-four patients (54%) had granulomatosis with polyangiitis. The main reasons for admission were respiratory failure (34%) and pulmonary-renal syndrome (33%). Mechanical ventilation was required in 51% of patients, catecholamines in 31%, and renal replacement therapy in 71%. Overall mortality at 90 days was 18% and the mortality in ICU was 16 %. The main causes of death in the ICU were disease flare in 69% and infection in 31%. In univariable analysis, relevant factors associated with death in nonsurvivors compared with survivors were Simplified Acute Physiology Score II (median [interquartile range] 51 [38-82] vs. 36 [27-42], p = 0.005), age (67 years [62-74] vs. 58 years [40-68], p < 0.003), Sequential Organ Failure Assessment score on the day of cyclophosphamide administration (11 [6-12] vs. 6 [3-7], p = 0.0004), and delayed administration of cyclophosphamide (5 days [3-14] vs. 2 days [1-5], p = 0.0053).
Patients admitted to the ICU for management of acute small-vessel vasculitis benefit from early, aggressive intensive care treatment, associated with an 18% death rate at 90 days.
因小血管炎急性发作入住重症监护病房(ICU)的患者的预后情况鲜有报道。本研究旨在确定因急性小血管炎入住ICU的患者的死亡率及预后因素。
本回顾性多中心研究于2001年1月至2014年12月在法国的20个ICU中进行。使用国际疾病分类第九版(ICD - 9)从各医院的计算机登记系统中识别患者。纳入标准为:(1)已知或高度怀疑患有肉芽肿性多血管炎、嗜酸性肉芽肿性多血管炎、显微镜下多血管炎(分别对应ICD - 9编码M31.3、M30.1和M31.7)或抗肾小球基底膜抗体病(ICD - 9编码N08.5X - 005或M31.0 +);(2)因血管炎急性发作入住ICU进行治疗;(3)在ICU内或入住ICU前48小时内接受环磷酰胺冲击治疗。主要终点是评估入住ICU 90天后的死亡率。
20个中心的82例患者被纳入研究,其中94%的患者近期(<6个月)被诊断为小血管炎。44例患者(54%)患有肉芽肿性多血管炎。入院的主要原因是呼吸衰竭(34%)和肺肾综合征(33%)。51%的患者需要机械通气,31%的患者需要使用儿茶酚胺,71%的患者需要进行肾脏替代治疗。90天的总体死亡率为18%,ICU内死亡率为16%。ICU内死亡的主要原因是疾病复发(69%)和感染(31%)。在单因素分析中,与幸存者相比,非幸存者死亡的相关因素有简化急性生理学评分II(中位数[四分位间距]51[38 - 82] vs. 36[27 - 42],p = 0.005)、年龄(67岁[62 - 74] vs. 58岁[40 - 68],p < 0.003)、环磷酰胺给药当天的序贯器官衰竭评估评分(11[6 - 12] vs. 6[3 - 7],p = 0.0004)以及环磷酰胺给药延迟(第5天[3 - 14] vs. 第2天[1 - 5],p = 0.0053)。
因急性小血管炎入住ICU的患者受益于早期积极的重症监护治疗,90天死亡率为18%。