Desai Roshni A, Davies Andrew L, Tachrount Mohamed, Kasti Marianne, Laulund Frida, Golay Xavier, Smith Kenneth J
Department of Neuroinflammation and Queen Square Multiple Sclerosis Centre, UCL Institute of Neurology, London, United Kingdom.
Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, London, United Kingdom.
Ann Neurol. 2016 Apr;79(4):591-604. doi: 10.1002/ana.24607. Epub 2016 Feb 22.
Demyelination is a cardinal feature of multiple sclerosis, but it remains unclear why new lesions form, and whether they can be prevented. Neuropathological evidence suggests that demyelination can occur in the relative absence of lymphocytes, and with distinctive characteristics suggestive of a tissue energy deficit. The objective was to examine an experimental model of the early multiple sclerosis lesion and identify pathogenic mechanisms and opportunities for therapy.
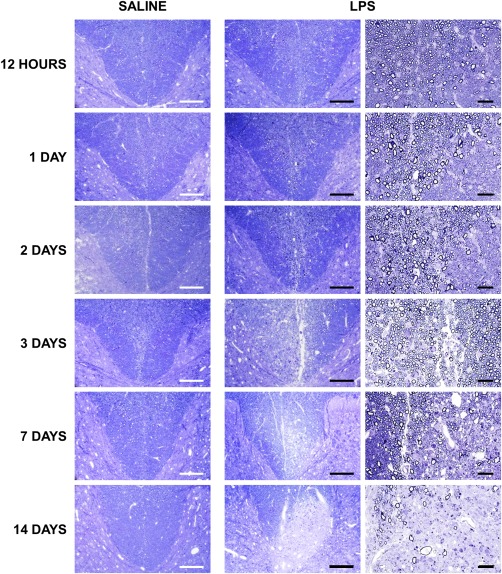
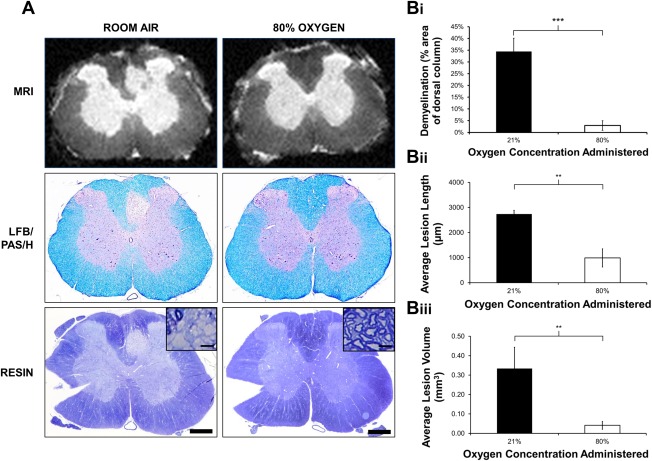
Demyelinating lesions were induced in the rat spinal dorsal column by microinjection of lipopolysaccharide, and examined immunohistochemically at different stages of development. The efficacy of treatment with inspired oxygen for 2 days following lesion induction was evaluated.
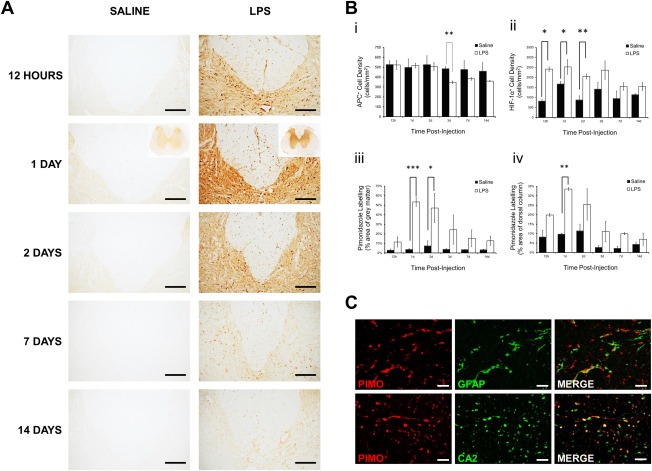
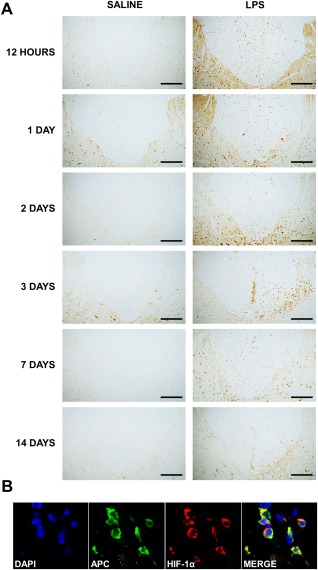
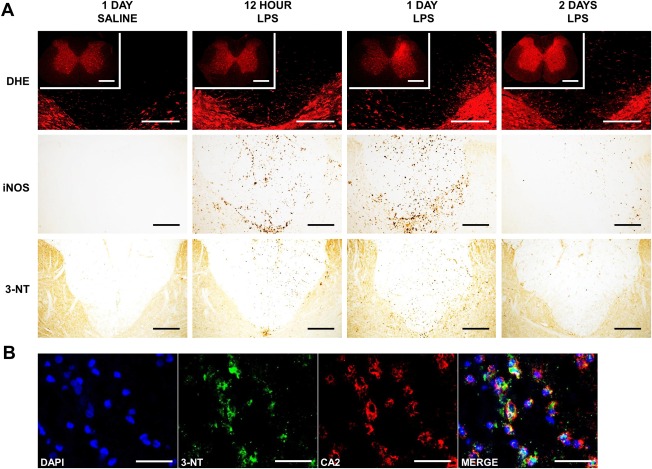
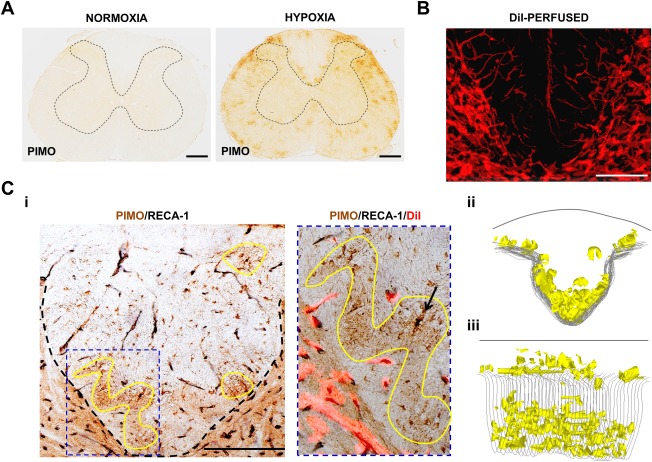
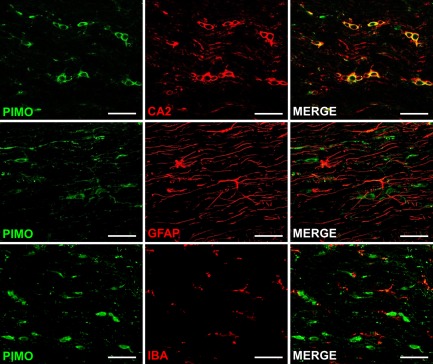
Demyelinating lesions were not centered on the injection site, but rather formed 1 week later at the white-gray matter border, preferentially including the ventral dorsal column watershed. Lesion formation was preceded by a transient early period of hypoxia and increased production of superoxide and nitric oxide. Oligodendrocyte numbers decreased at the site shortly afterward, prior to demyelination. Lesions formed at a site of inherent susceptibility to hypoxia, as revealed by exposure of naive animals to a hypoxic environment. Notably, raising the inspired oxygen (80%, normobaric) during the hypoxic period significantly reduced or prevented the demyelination.
Demyelination characteristic of at least some early multiple sclerosis lesions can arise at a vascular watershed following activation of innate immune mechanisms that provoke hypoxia, and superoxide and nitric oxide formation, all of which can compromise cellular energy sufficiency. Demyelination can be reduced or eliminated by increasing inspired oxygen to alleviate the transient hypoxia.
脱髓鞘是多发性硬化的主要特征,但新病灶为何形成以及能否预防仍不清楚。神经病理学证据表明,脱髓鞘可在淋巴细胞相对缺乏的情况下发生,且具有提示组织能量不足的独特特征。目的是研究早期多发性硬化病灶的实验模型,并确定致病机制和治疗机会。
通过微量注射脂多糖在大鼠脊髓背柱诱导脱髓鞘病灶,并在不同发育阶段进行免疫组织化学检查。评估病灶诱导后吸入氧气治疗2天的疗效。
脱髓鞘病灶并非以注射部位为中心,而是在1周后于白质-灰质边界形成,优先累及腹侧背柱分水岭区。病灶形成之前有一段短暂的早期缺氧期,超氧化物和一氧化氮的产生增加。随后不久,在脱髓鞘之前,少突胶质细胞数量在该部位减少。正如将未接触过缺氧环境的动物暴露于缺氧环境所显示的那样,病灶在对缺氧具有固有易感性的部位形成。值得注意的是,在缺氧期提高吸入氧气(常压下80%)可显著减少或预防脱髓鞘。
至少一些早期多发性硬化病灶的脱髓鞘特征可在先天免疫机制激活引发缺氧、超氧化物和一氧化氮形成后,于血管分水岭区出现,所有这些都可能损害细胞能量充足性。通过增加吸入氧气以缓解短暂缺氧,可减少或消除脱髓鞘。