Boettiger David C, Aurpibul Linda, Hudaya Dina Mukiarti, Fong Siew M, Lumbiganon Pagakrong, Saphonn Vonthanak, Truong Khanh H, Hansudewechakul Rawiwan, Nguyen Lam V, Do Viet C, Bunupuradah Torsak, Chokephaibulkit Kulkanya, Nik Yusoff Nik Khairulddin, Kumarasamy Nagalingeswaran, Wati Dewi Kumara, Razali Kamarul Azahar, Kariminia Azar
From the *The Kirby Institute, UNSW Australia, Sydney, Australia; †Department of Pediatrics, Faculty of Medicine, Chiang Mai University and Research Institute for Health Sciences, Chiang Mai, Thailand; ‡Cipto Mangunkusumo General Hospital, Jakarta, Indonesia; §Hospital Likas, Kota Kinabalu, Malaysia; ¶Division of Infectious Diseases, Department of Pediatrics, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; ‖National Centre for HIV/AIDS Dermatology and STDs, Phnom Penh, Cambodia; **Children's Hospital 1, Ho Chi Minh City, Vietnam; ††Chiangrai Prachanukroh Hospital, Chiang Rai, Thailand; ‡‡National Hospital of Pediatrics, Hanoi, Vietnam; §§Children's Hospital 2, Ho Chi Minh City, Vietnam; ¶¶HIV-NAT, the Thai Red Cross AIDS Research Centre, Bangkok, Thailand; ‖‖Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; ***Hospital Raja Perempuan Zainab II, Kelantan, Malaysia; †††YRGCARE Medical Centre, CART CRS, Chennai, India; ‡‡‡Sanglah Hospital, Udayana University, Bali, Indonesia; §§§Pediatric Institute, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia; and ¶¶¶Members of TREAT Asia Pediatric HIV Observational Database are listed in Appendix.
Pediatr Infect Dis J. 2016 May;35(5):e144-51. doi: 10.1097/INF.0000000000001074.
Information on antiretroviral therapy (ART) use in HIV-infected children with severe malnutrition (SM) is lacking. We investigated long-term ART outcomes in this population.
Children enrolled in the TREAT Asia Pediatric HIV Observational Database who had SM (weight-for-height or body mass index-for-age Z score less than -3) at ART initiation were analyzed. Generalized estimating equations were used to investigate poor weight recovery (weight-for-age Z score less than -3) and poor CD4% recovery (CD4% <25), and competing risk regression was used to analyze mortality and toxicity-associated treatment modification.
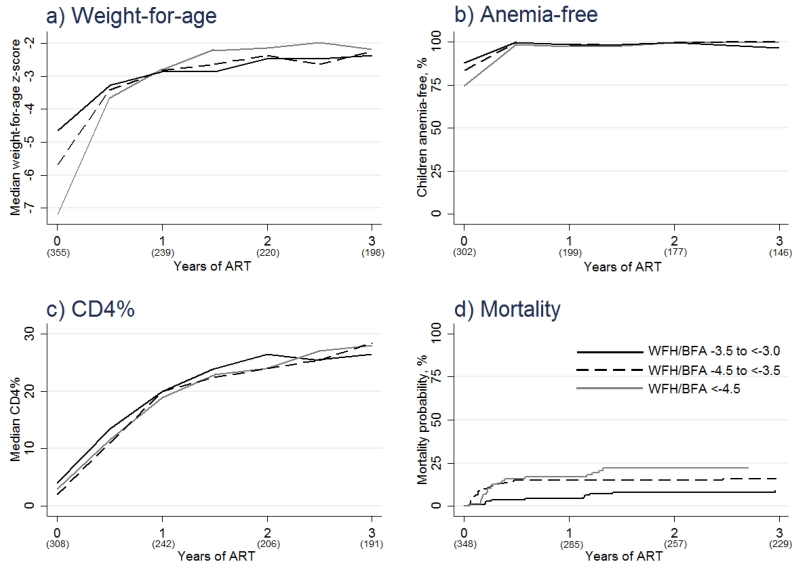
Three hundred fifty-five (11.9%) of 2993 children starting ART had SM. Their median weight-for-age Z score increased from -5.6 at ART initiation to -2.3 after 36 months. Not using trimethoprim-sulfamethoxazole prophylaxis at baseline was associated with poor weight recovery [odds ratio: 2.49 vs. using; 95% confidence interval (CI): 1.66-3.74; P < 0.001]. Median CD4% increased from 3.0 at ART initiation to 27.2 after 36 months, and 56 (15.3%) children died during follow-up. More profound SM was associated with poor CD4% recovery (odds ratio: 1.78 for Z score less than -4.5 vs. -3.5 to less than -3.0; 95% CI: 1.08-2.92; P = 0.023) and mortality (hazard ratio: 2.57 for Z score less than -4.5 vs. -3.5 to less than -3.0; 95% CI: 1.24-5.33; P = 0.011). Twenty-two toxicity-associated ART modifications occurred at a rate of 2.4 per 100 patient-years, and rates did not differ by malnutrition severity.
Trimethoprim-sulfamethoxazole prophylaxis is important for the recovery of weight-for-age in severely malnourished children starting ART. The extent of SM does not impede weight-for-age recovery or antiretroviral tolerability, but CD4% response is compromised in children with a very low weight-for-height/body mass index-for-age Z score, which may contribute to their high rate of mortality.
缺乏关于感染人类免疫缺陷病毒(HIV)且患有重度营养不良(SM)儿童抗逆转录病毒疗法(ART)使用情况的信息。我们调查了该人群ART的长期疗效。
对亚洲治疗儿童HIV观察数据库中在开始ART时患有SM(身高别体重或年龄别体质指数Z评分低于-3)的儿童进行分析。采用广义估计方程研究体重恢复不佳(年龄别体重Z评分低于-3)和CD4%恢复不佳(CD4%<25)情况,并使用竞争风险回归分析死亡率和与毒性相关的治疗调整。
2993名开始ART的儿童中有355名(11.9%)患有SM。他们的年龄别体重Z评分中位数从开始ART时的-5.6增加到36个月后的-2.3。基线时未使用甲氧苄啶-磺胺甲恶唑预防与体重恢复不佳相关[比值比:2.49 vs. 使用;95%置信区间(CI):1.66-3.74;P<0.001]。CD4%中位数从开始ART时的3.0增加到36个月后的27.2,56名(15.3%)儿童在随访期间死亡。更严重的SM与CD4%恢复不佳(比值比:Z评分低于-4.5时为1.78,而-3.5至低于-3.0时为1.08-2.92;P = 0.023)和死亡率(风险比:Z评分低于-4.5时为2.57,而-3.5至低于-3.0时为1.24-5.33;P = 0.011)相关。发生了22次与毒性相关的ART调整,发生率为每100患者年2.4次,且发生率在营养不良严重程度之间无差异。
甲氧苄啶-磺胺甲恶唑预防对于开始ART的重度营养不良儿童的年龄别体重恢复很重要。SM的程度不妨碍年龄别体重恢复或抗逆转录病毒耐受性,但身高别体重/年龄别体质指数Z评分极低的儿童CD4%反应受损,这可能导致其高死亡率。