Lai Yinzhi, Wang Chun, Civan Jesse M, Palazzo Juan P, Ye Zhong, Hyslop Terry, Lin Jianqing, Myers Ronald E, Li Bingshan, Jiang Binghua, Sama Ashwin, Xing Jinliang, Yang Hushan
Division of Population Science, Department of Medical Oncology, Sidney Kimmel Cancer Center, Thomas Jefferson University, Philadelphia, Pennsylvania.
Division of Gastroenterology and Hepatology, Department of Medicine, Thomas Jefferson University, Philadelphia, Pennsylvania.
Gastroenterology. 2016 May;150(5):1135-1146. doi: 10.1053/j.gastro.2016.01.030. Epub 2016 Feb 2.
BACKGROUND & AIMS: We evaluated differences in treatment of black vs white patients with colon cancer and assessed their effects on survival, based on cancer stage.
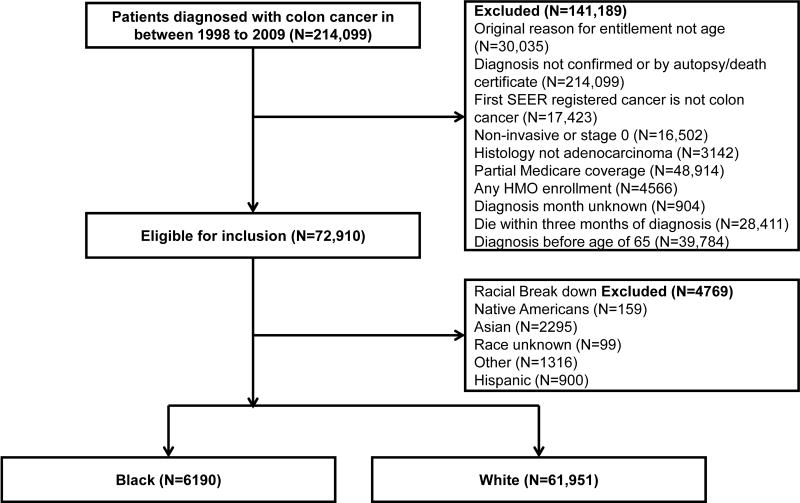
We collected data from the Surveillance, Epidemiology, and End Results-Medicare database and identified 6190 black and 61,951 white patients with colon cancer diagnosed from 1998 through 2009 and followed up through 2011. Three sets of 6190 white patients were matched sequentially, using a minimum distance strategy, to the same set of 6190 black patients based on demographic (age; sex; diagnosis year; and Surveillance, Epidemiology, and End Results registry), tumor presentation (demographic plus comorbidities, tumor stage, grade, and size), and treatment (presentation plus therapies) variables. We conducted sensitivity analyses to explore the effects of socioeconomic status in a subcohort that included 2000 randomly selected black patients. Racial differences in treatment were assessed using a logistic regression model; their effects on racial survival disparity were evaluated using the Kaplan-Meier method and the Cox proportional hazards model.
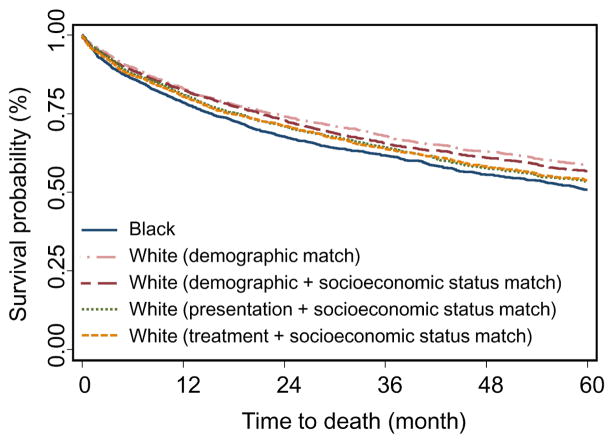
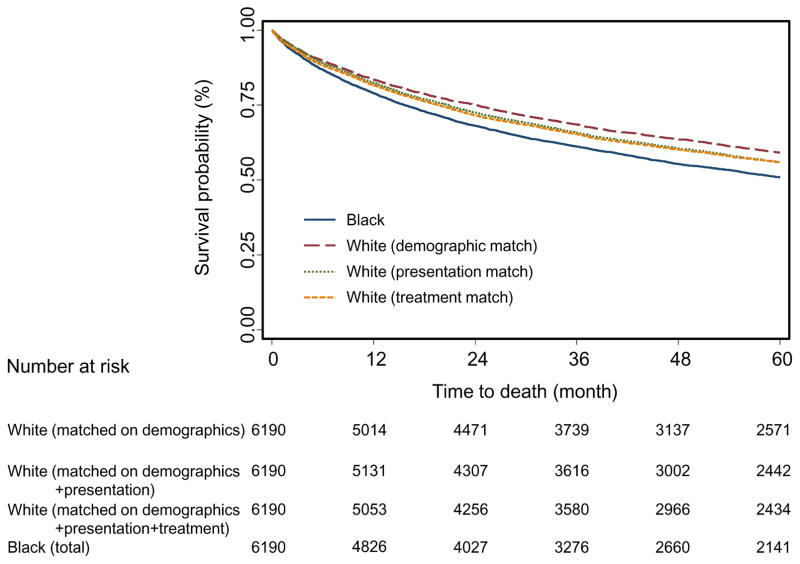
After patients were matched for demographic variables, the absolute 5-year difference in survival between black and white patients was 8.3% (white, 59.2% 5-y survival; blacks, 50.9% 5-y survival) (P < .0001); this value decreased significantly, to 5.0% (P < .0001), after patients were matched for tumor presentation, and decreased to 4.9% (P < .0001) when patients were matched for treatment. Differences in treatment therefore accounted for 0.1% of the 8.3% difference in survival between black and white patients. After patients were matched for tumor presentation, racial disparities were observed in almost all types of treatment; the disparities were most prominent for patients with advanced-stage cancer (stages III or IV, up to an 11.1% difference) vs early stage cancer (stages I or II, up to a 4.3% difference). After patients were matched for treatment, there was a greater reduction in disparity for black vs white patients with advanced-stage compared with early-stage cancer. In sensitivity analyses, the 5-year racial survival disparity was 7.7% after demographic match, which was less than the 8.3% observed in the complete cohort. This reduction likely was owing to the differences between the subcohort and the complete cohort in those variables that were not included in the demographic match. This value was reduced to 6.5% (P = .0001) after socioeconomic status was included in the demographic match. The difference decreased significantly to 2.8% (P = .090) after tumor presentation match, but was not reduced further after treatment match.
We observed significant disparities in treatment and survival of black vs white patients with colon cancer. The disparity in survival appears to have been affected more strongly by tumor presentation at diagnosis than treatment. The effects of treatment differences on disparities in survival were greater for patients with advanced-stage vs early-stage cancer.
我们评估了黑种人与白种人结肠癌患者在治疗上的差异,并根据癌症分期评估了这些差异对生存率的影响。
我们从监测、流行病学和最终结果-医疗保险数据库收集数据,确定了1998年至2009年诊断出的6190例黑种人和61951例白种人结肠癌患者,并随访至2011年。基于人口统计学(年龄、性别、诊断年份以及监测、流行病学和最终结果登记处)、肿瘤特征(人口统计学加上合并症、肿瘤分期、分级和大小)以及治疗(特征加上治疗方法)变量,采用最小距离策略,将三组各6190例白种患者依次与同一组6190例黑种患者进行匹配。我们在一个包含2000例随机选择的黑种患者的亚组中进行敏感性分析,以探讨社会经济地位的影响。使用逻辑回归模型评估治疗方面的种族差异;使用Kaplan-Meier方法和Cox比例风险模型评估其对种族生存差异的影响。
在患者按人口统计学变量匹配后,黑种人和白种人患者5年生存率的绝对差异为8.3%(白种人5年生存率为59.2%;黑种人5年生存率为50.9%)(P <.0001);在患者按肿瘤特征匹配后,该值显著降至5.0%(P <.0001),在患者按治疗匹配后降至4.9%(P <.0001)。因此,治疗差异占黑种人和白种人患者8.3%的生存差异的0.1%。在患者按肿瘤特征匹配后,几乎所有类型的治疗中都观察到了种族差异;晚期癌症(III期或IV期,差异高达11.1%)与早期癌症(I期或II期,差异高达4.3%)患者之间的差异最为显著。在患者按治疗匹配后,晚期癌症的黑种人与白种人患者之间的差异比早期癌症患者的差异减少得更多。在敏感性分析中,人口统计学匹配后5年的种族生存差异为7.7%,低于整个队列中观察到的8.3%。这种降低可能是由于亚组与整个队列在人口统计学匹配中未包括的那些变量方面存在差异。在人口统计学匹配中纳入社会经济地位后,该值降至6.5%(P =.0001)。在肿瘤特征匹配后,差异显著降至2.8%(P =.090),但在治疗匹配后未进一步降低。
我们观察到黑种人与白种人结肠癌患者在治疗和生存方面存在显著差异。生存差异似乎在更大程度上受到诊断时肿瘤特征的影响,而非治疗。治疗差异对生存差异的影响在晚期癌症患者中比早期癌症患者更大。