Choi Eun Ji, Choi Yun Mi, Jang Eun Jung, Kim Ju Yeon, Kim Tae Kyun, Kim Kyung Hoon
Department of Anesthesia and Pain Medicine, School of Medicine, Pusan National University, Yangsan, Korea.
Korean J Pain. 2016 Jan;29(1):3-11. doi: 10.3344/kjp.2016.29.1.3. Epub 2016 Jan 4.
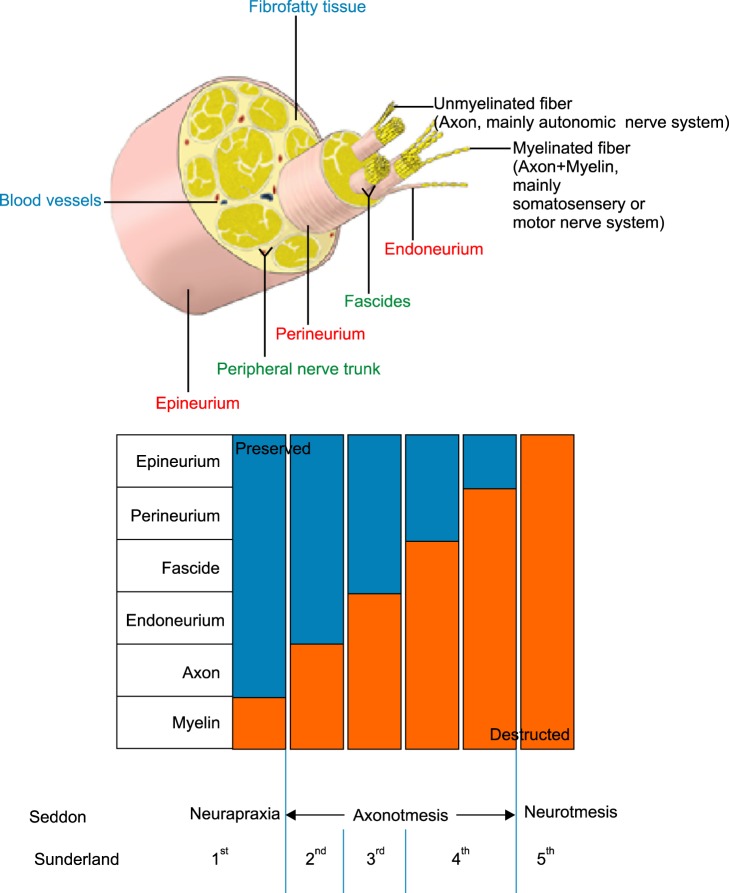
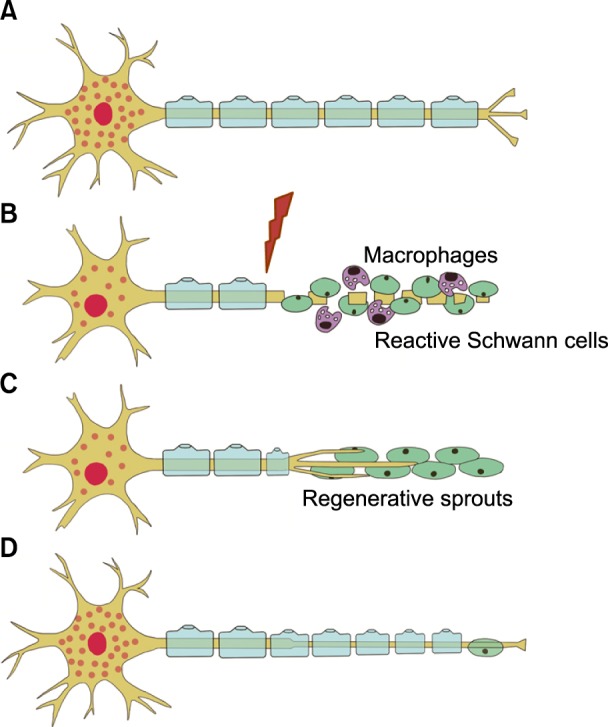
A nerve block is an effective tool for diagnostic and therapeutic methods. If a diagnostic nerve block is successful for pain relief and the subsequent therapeutic nerve block is effective for only a limited duration, the next step that should be considered is a nerve ablation or modulation. The nerve ablation causes iatrogenic neural degeneration aiming only for sensory or sympathetic denervation without motor deficits. Nerve ablation produces the interruption of axonal continuity, degeneration of nerve fibers distal to the lesion (Wallerian degeneration), and the eventual death of axotomized neurons. The nerve ablation methods currently available for resection/removal of innervation are performed by either chemical or thermal ablation. Meanwhile, the nerve modulation method for interruption of innervation is performed using an electromagnetic field of pulsed radiofrequency. According to Sunderland's classification, it is first and foremost suggested that current neural ablations produce third degree peripheral nerve injury (PNI) to the myelin, axon, and endoneurium without any disruption of the fascicular arrangement, perineurium, and epineurium. The merit of Sunderland's third degree PNI is to produce a reversible injury. However, its shortcoming is the recurrence of pain and the necessity of repeated ablative procedures. The molecular mechanisms related to axonal regeneration after injury include cross-talk between axons and glial cells, neurotrophic factors, extracellular matrix molecules, and their receptors. It is essential to establish a safe, long-standing denervation method without any complications in future practices based on the mechanisms of nerve degeneration as well as following regeneration.
神经阻滞是诊断和治疗方法的一种有效工具。如果诊断性神经阻滞成功缓解疼痛,而后续的治疗性神经阻滞仅在有限时间内有效,那么接下来应考虑的步骤是神经消融或调节。神经消融导致医源性神经变性,仅旨在实现感觉或交感神经去神经支配而不产生运动功能障碍。神经消融会导致轴突连续性中断、病变远端神经纤维变性(沃勒变性)以及轴突切断的神经元最终死亡。目前可用于切除/去除神经支配的神经消融方法通过化学或热消融来进行。同时,用于中断神经支配的神经调节方法是使用脉冲射频的电磁场来实施。根据桑德兰分类法,首先需要指出的是,当前的神经消融会对髓鞘、轴突和神经内膜造成三度周围神经损伤(PNI),而束状排列、神经束膜和神经外膜不会受到任何破坏。桑德兰三度PNI的优点是产生可逆性损伤。然而,其缺点是疼痛复发以及需要重复进行消融手术。与损伤后轴突再生相关的分子机制包括轴突与神经胶质细胞之间的相互作用、神经营养因子、细胞外基质分子及其受体。基于神经变性以及后续再生的机制,在未来的实践中建立一种安全、长期且无任何并发症的去神经支配方法至关重要。