Holter Jan C, Ueland Thor, Jenum Pål A, Müller Fredrik, Brunborg Cathrine, Frøland Stig S, Aukrust Pål, Husebye Einar, Heggelund Lars
Department of Internal Medicine, Drammen Hospital, Vestre Viken Health Trust, Drammen, Norway.
Research Institute of Internal Medicine, Oslo University Hospital Rikshospitalet, Oslo, Norway.
PLoS One. 2016 Feb 5;11(2):e0148741. doi: 10.1371/journal.pone.0148741. eCollection 2016.
Contributors to long-term mortality in patients with community-acquired pneumonia (CAP) remain unclear, with little attention paid to pneumonia etiology. We examined long-term survival, causes of death, and risk factors for long-term mortality in adult patients who had been hospitalized for CAP, with emphasis on demographic, clinical, laboratory, and microbiological characteristics.
Two hundred and sixty-seven consecutive patients admitted in 2008-2011 to a general hospital with CAP were prospectively recruited and followed up. Patients who died during hospital stay were excluded. Demographic, clinical, and laboratory data were collected within 48 hours of admission. Extensive microbiological work-up was performed to establish the etiology of CAP in 63% of patients. Mortality data were obtained from the Norwegian Cause of Death Registry. Cox regression models were used to identify independent risk factors for all-cause mortality.
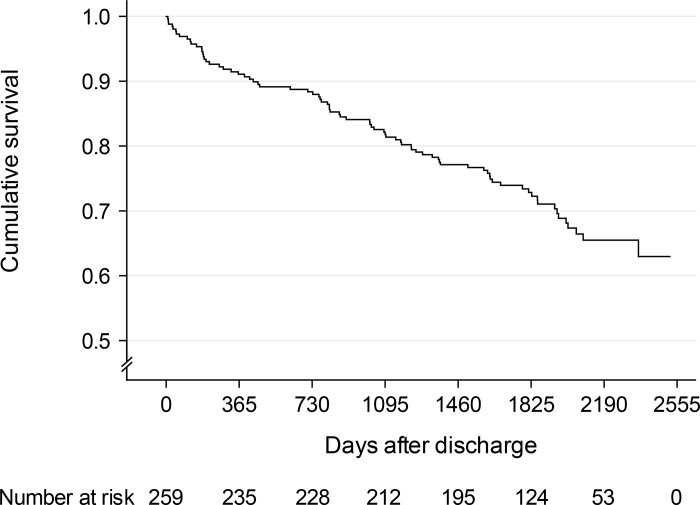
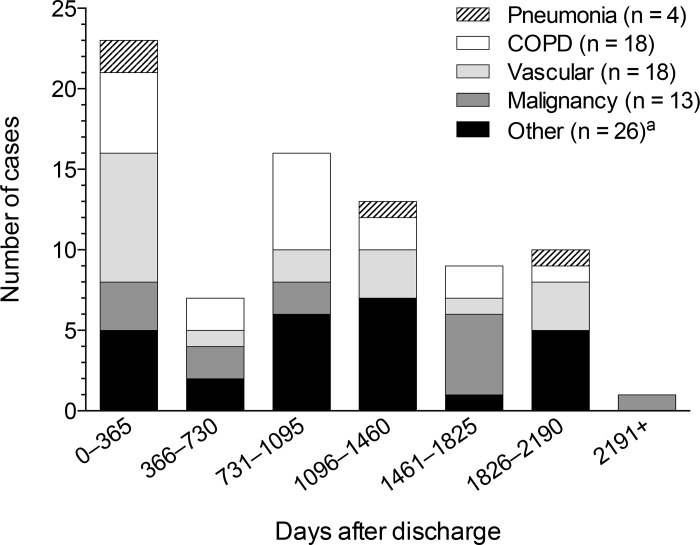
Of 259 hospital survivors of CAP (median age 66 years), 79 (30.5%) died over a median of 1,804 days (range 1-2,520 days). Cumulative 5-year survival rate was 72.9% (95% CI 67.4-78.4%). Standardized mortality ratio was 2.90 for men and 2.05 for women. The main causes of death were chronic obstructive pulmonary disease (COPD), vascular diseases, and malignancy. Independent risk factors for death were the following (hazard ratio, 95% CI): age (1.83 per decade, 1.47-2.28), cardiovascular disease (2.63, 1.61-4.32), COPD (2.09, 1.27-3.45), immunocompromization (1.98, 1.17-3.37), and low serum albumin level at admission (0.75 per 5 g/L higher, 0.58-0.96), whereas active smoking was protective (0.32, 0.14-0.74); active smokers were younger than non-smokers (P < 0.001). Microbial etiology did not predict mortality.
Results largely confirm substantial comorbidity-related 5-year mortality after hospitalization for CAP and the impact of several well-known risk factors for death, and extend previous findings on the prognostic value of serum albumin level at hospital admission. Pneumonia etiology had no prognostic value, but this remains to be substantiated by further studies using extensive diagnostic microbiological methods in the identification of causative agents of CAP.
社区获得性肺炎(CAP)患者长期死亡率的影响因素尚不清楚,且很少有人关注肺炎的病因。我们研究了因CAP住院的成年患者的长期生存情况、死亡原因及长期死亡的危险因素,重点关注人口统计学、临床、实验室和微生物学特征。
前瞻性招募并随访了2008年至2011年期间连续入住一家综合医院的267例CAP患者。排除住院期间死亡的患者。在入院48小时内收集人口统计学、临床和实验室数据。对63%的患者进行了广泛的微生物学检查以确定CAP的病因。死亡率数据来自挪威死亡原因登记处。采用Cox回归模型确定全因死亡率的独立危险因素。
259例CAP住院存活患者(中位年龄66岁)中,79例(30.5%)在中位1804天(范围1 - 2520天)内死亡。5年累积生存率为72.9%(95%可信区间67.4 - 78.)。男性标准化死亡率为2.90,女性为2.05。主要死亡原因是慢性阻塞性肺疾病(COPD)、血管疾病和恶性肿瘤。死亡的独立危险因素如下(风险比,95%可信区间):年龄(每增加十岁1.83,1.47 - 2.28)、心血管疾病(2.63,1.61 - 4.32)、COPD(2.09,1.27 - 3.45)、免疫功能低下(1.98,1.17 - 3.37)以及入院时低血清白蛋白水平(每高5 g/L为0.75,0.58 - 0.96),而当前吸烟具有保护作用(0.32,0.14 - 0.74);当前吸烟者比非吸烟者年轻(P < 0.001)。微生物病因不能预测死亡率。
结果在很大程度上证实了CAP住院后与合并症相关的5年死亡率以及几种已知死亡危险因素的影响,并扩展了先前关于入院时血清白蛋白水平预后价值的研究结果。肺炎病因没有预后价值,但这仍有待通过在CAP病原体鉴定中使用广泛诊断微生物学方法的进一步研究来证实。