Bellew Shawna D, Bremer Merri L, Kopecky Stephen L, Lohse Christine M, Munger Thomas M, Robelia Paul M, Smars Peter A
Department of Emergency Medicine, Mayo Clinic, Rochester, MN.
Division of Cardiovascular Diseases, Mayo Clinic, Rochester, MN.
J Am Heart Assoc. 2016 Feb 8;5(2):e002984. doi: 10.1161/JAHA.115.002984.
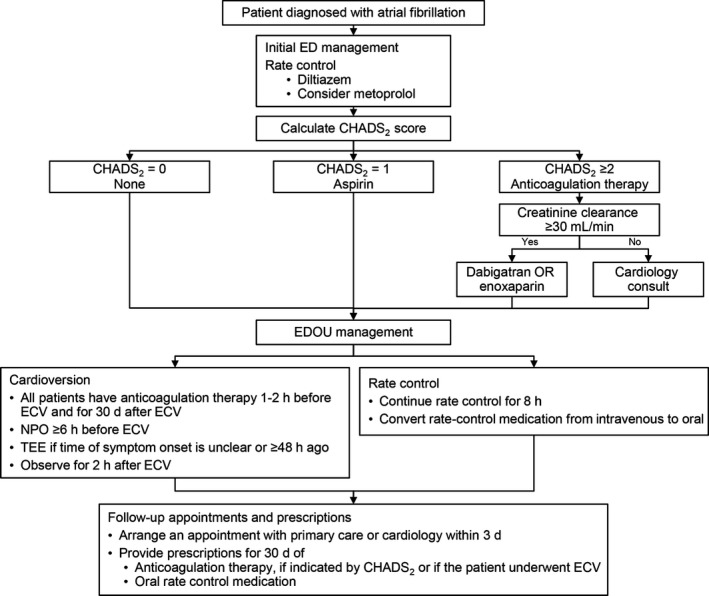
Atrial fibrillation (AF) is a common, growing, and costly medical condition. We aimed to evaluate the impact of a management algorithm for symptomatic AF that used an emergency department observation unit on hospital admission rates and patient outcomes.
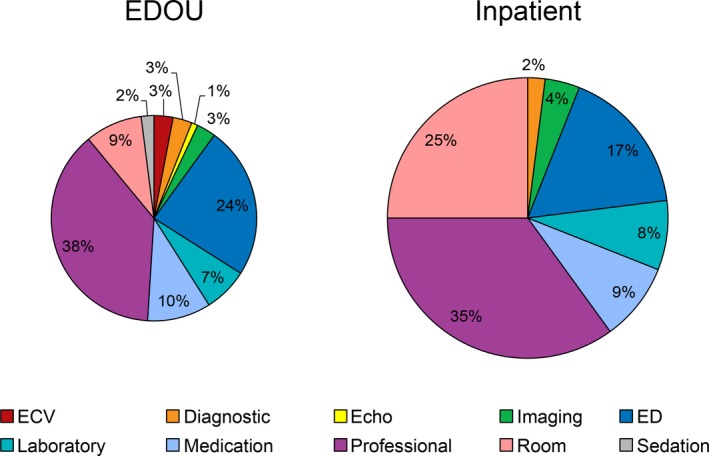
This retrospective cohort study compared 563 patients who presented consecutively in the year after implementation of the algorithm, from July 2013 through June 2014 (intervention group), with 627 patients in a historical cohort (preintervention group) who presented consecutively from July 2011 through June 2012. All patients who consented to have their records used for chart review were included if they had a primary final emergency department diagnosis of AF. We observed no significant differences in age, sex, vital signs, body mass index, or CHADS2 (congestive heart failure, hypertension, age, diabetes mellitus, and prior stroke or transient ischemic attack) score between the preintervention and intervention groups. The rate of inpatient admission was significantly lower in the intervention group (from 45% to 36%; P<0.001). The groups were not significantly different with regard to rates of return emergency department visits (19% versus 17%; P=0.48), hospitalization (18% versus 16%; P=0.22), or adverse events (2% versus 2%; P=0.95) within 30 days. Emergency department observation unit admissions were 40% (P<0.001) less costly than inpatient hospital admissions of ≤1 day's duration.
Implementation of an emergency department observation unit AF algorithm was associated with significantly decreased hospital admissions without increasing the rates of return emergency department visits, hospitalization, or adverse events within 30 days.
心房颤动(AF)是一种常见、不断增加且费用高昂的病症。我们旨在评估一种用于有症状AF的管理算法的影响,该算法使用急诊科观察单元对住院率和患者结局的影响。
这项回顾性队列研究将2013年7月至2014年6月算法实施后连续就诊的563例患者(干预组)与2011年7月至2012年6月历史队列中的627例连续就诊患者(干预前组)进行了比较。所有同意将其记录用于病历审查的患者,若其急诊科最终主要诊断为AF,则纳入研究。我们观察到干预前组和干预组在年龄、性别、生命体征、体重指数或CHADS2(充血性心力衰竭、高血压、年龄、糖尿病以及既往卒中或短暂性脑缺血发作)评分方面无显著差异。干预组的住院率显著降低(从45%降至36%;P<0.001)。两组在30天内的急诊复诊率(19%对17%;P=0.48)、住院率(18%对16%;P=0.22)或不良事件发生率(2%对2%;P=0.95)方面无显著差异。急诊科观察单元住院费用比住院时间≤1天的住院费用低40%(P<0.001)。
实施急诊科观察单元房颤算法与住院率显著降低相关,且未增加30天内的急诊复诊率、住院率或不良事件发生率。