Spaetgens Bart, Pustjens Tobias, Scheepers Lieke E J M, Janssens Hein J E M, van der Linden Sjef, Boonen Annelies
Department of Internal Medicine, Division of Rheumatology, Maastricht University Medical Centre, P.O. Box 5800, 6202 AZ, Maastricht, The Netherlands.
CAPHRI Research Institute, University Maastricht, Maastricht, The Netherlands.
Clin Rheumatol. 2016 Aug;35(8):2053-2061. doi: 10.1007/s10067-016-3212-2. Epub 2016 Feb 22.
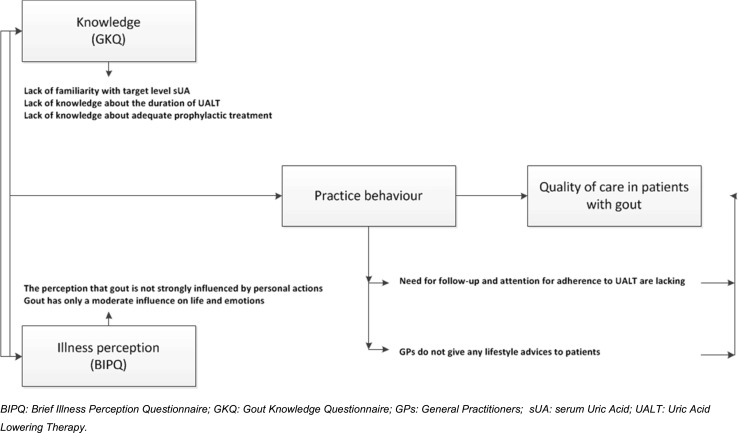
The objective of the present study is to explore knowledge, illness perceptions and stated practice behaviour in relation to gout in primary care. This is a mixed methods study among 32 general practitioners (GPs). The quantitative assessment included the Gout Knowledge Questionnaire (GKQ; range 0-10; better) and Brief Illness Perceptions Questionnaire (BIPQ; nine items, range 0-10; stronger). Structured individual interviews obtained further qualitative insight into knowledge and perceptions, in the context of daily practice. Among 32 GPs, 18 (56.3 %) were male, mean age 44.4 years (SD 9.6) and mean working experience 17.1 years (SD 9.7). Median score [interquartile ranges (IQR)] on the GKQ was 7.8 [6.7-8.9] and 9.0 [8.0-10.0], when presented as open or multiple-choice questions, respectively. The BIPQ (median; [IQR]) revealed that gout was seen as a chronic disease (8.0; [7.0-9.0]), affecting life and emotions moderately (6.5; [5.0-7.0]), having many severe symptoms (8.0; [7.0-9.0]) and in which treatment could be very helpful (8.0; [7.0-9.0]). Further interviews revealed large variation in specific aspects of knowledge and about gaps concerning indications for uric acid-lowering therapy (UALT), duration of UALT, target serum uric acid (sUA) level or duration of prophylactic treatment. Finally, patients' adherence was not checked systematically. Specific knowledge gaps and discrepancies between perceptions and stated practice behaviour were identified, which might hamper effective management of this well-treatable disease. Improving evidence on the rationale and effectiveness of treatment targets and adherence interventions, tailoring guidelines to general practice and intensification of implementation of guidelines in primary health care seem to be needed.
本研究的目的是探讨基层医疗中与痛风相关的知识、疾病认知及既定的实践行为。这是一项针对32名全科医生(GP)的混合方法研究。定量评估包括痛风知识问卷(GKQ;范围0 - 10分,分数越高越好)和简短疾病认知问卷(BIPQ;九个项目,范围0 - 10分,分数越高认知越强)。结构化的个人访谈在日常实践背景下,进一步深入了解了知识和认知情况。在32名全科医生中,18名(56.3%)为男性,平均年龄44.4岁(标准差9.6),平均工作经验17.1年(标准差9.7)。当以开放式或多项选择题形式呈现时,GKQ的中位数得分[四分位间距(IQR)]分别为7.8[6.7 - 8.9]和9.0[8.0 - 10.0]。BIPQ(中位数;[IQR])显示,痛风被视为一种慢性疾病(8.0;[7.0 - 9.0]),对生活和情绪有中度影响(6.5;[5.0 - 7.0]),有许多严重症状(8.0;[7.0 - 9.0]),且治疗可能非常有帮助(8.0;[7.0 - 9.0])。进一步访谈发现,在知识的具体方面以及关于降尿酸治疗(UALT)指征、UALT持续时间、目标血清尿酸(sUA)水平或预防性治疗持续时间的差距方面存在很大差异。最后,未系统检查患者的依从性。确定了具体的知识差距以及认知与既定实践行为之间的差异,这可能会妨碍对这种可有效治疗疾病的有效管理。似乎需要改进关于治疗目标和依从性干预的基本原理及有效性的证据,使指南更适合基层医疗实践,并加强在初级卫生保健中指南的实施。