Burns D M, Rana S, Martin E, Nagra S, Ward J, Osman H, Bell A I, Moss P, Russell N H, Craddock C F, Fox C P, Chaganti S
Institute of Cancer and Genomic Sciences, University of Birmingham, Birmingham, UK.
Centre for Clinical Haematology, University Hospitals Birmingham NHS Trust, Birmingham, UK.
Bone Marrow Transplant. 2016 Jun;51(6):825-32. doi: 10.1038/bmt.2016.19. Epub 2016 Feb 22.
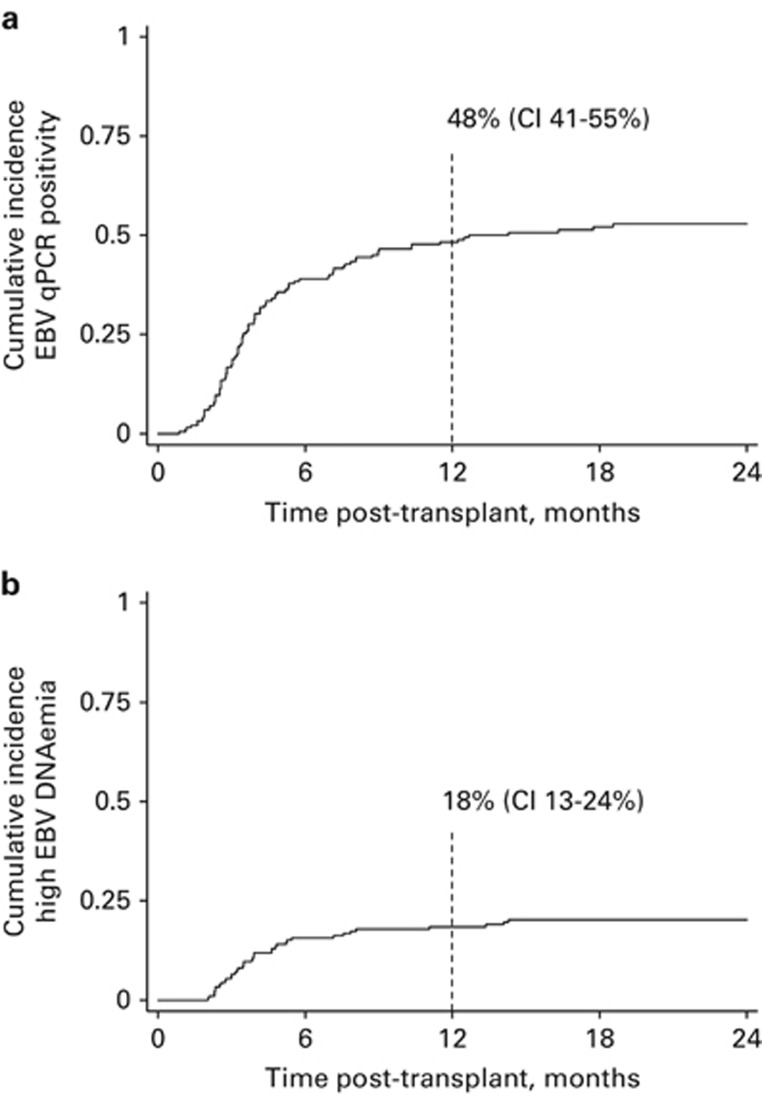
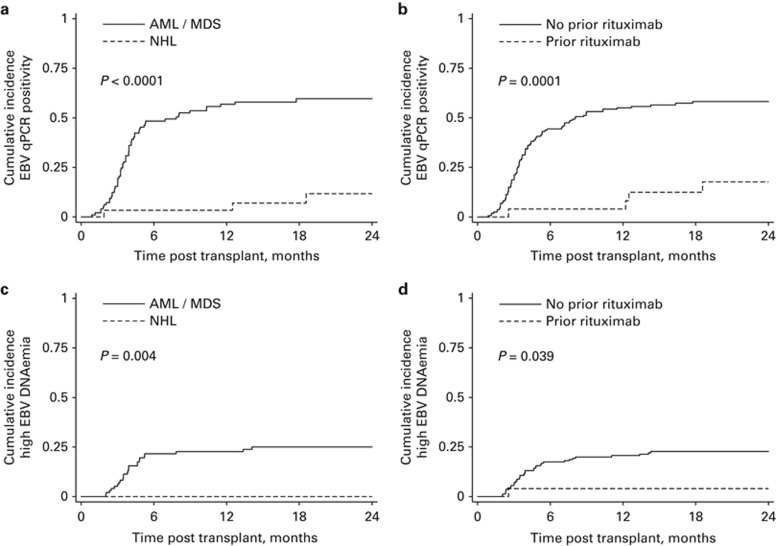
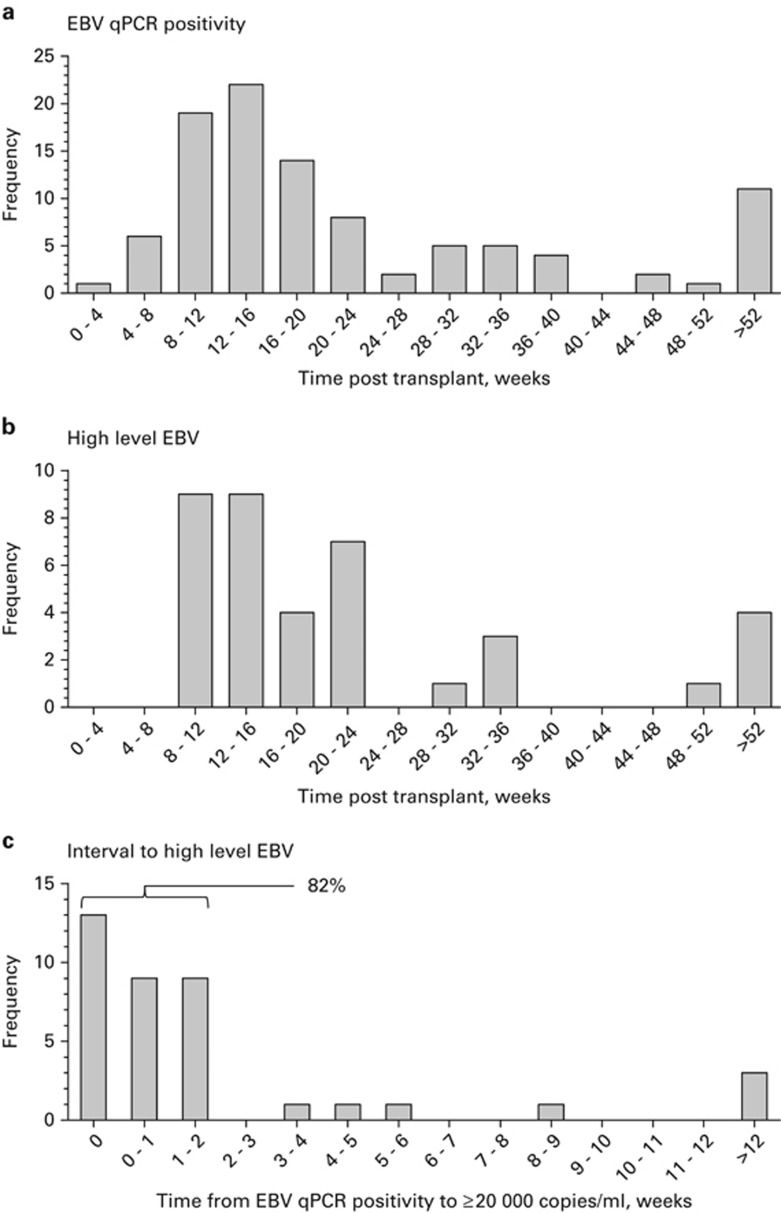
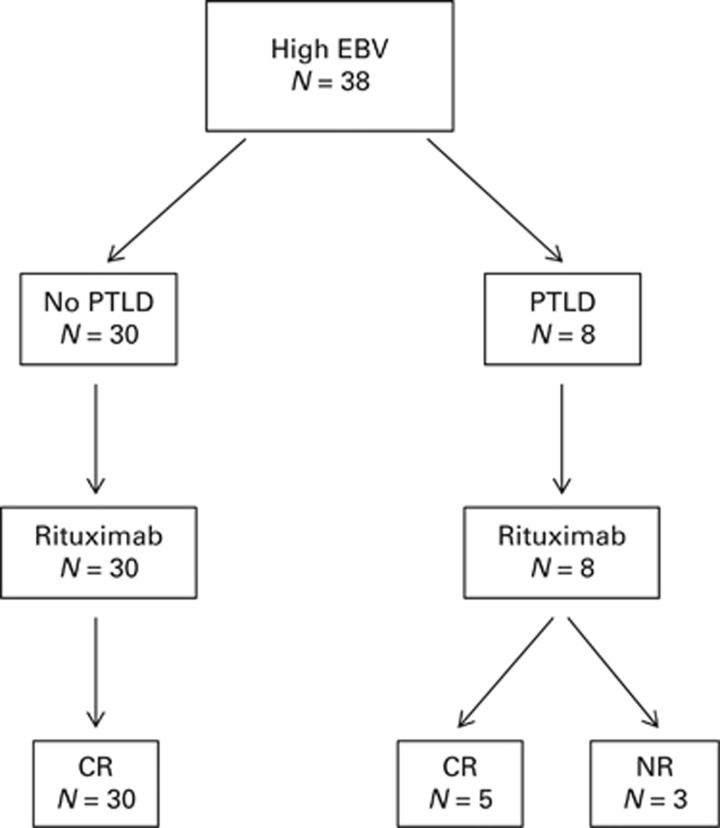
EBV-associated post-transplant lymphoproliferative disease (PTLD) remains an important complication of allogeneic haematopoietic stem cell transplantation (allo-HSCT). We retrospectively analysed the incidence and risk factors for EBV reactivation in 186 adult patients undergoing consecutive allo-HSCT with alemtuzumab T-cell depletion at a single centre. The cumulative incidence of EBV reactivation was 48% (confidence interval (CI) 41-55%) by 1 year, with an incidence of high-level EBV reactivation of 18% (CI 13-24%); 8 patients were concurrently diagnosed with PTLD. Amongst patients with high-level reactivation 31/38 (82%) developed this within only 2 weeks of first EBV qPCR positivity. In univariate analysis age⩾50 years was associated with significantly increased risk of EBV reactivation (hazard ratio (HR) 1.54, CI 1.02-2.31; P=0.039). Furthermore, a diagnosis of non-Hodgkin lymphoma (NHL) was associated with greatly reduced risk of reactivation (HR 0.10, CI 0.03-0.33; P=0.0001) and this was confirmed in multivariate testing. Importantly, rituximab therapy within 6 months prior to allo-HSCT was also highly predictive for lack of EBV reactivation (HR 0.18, CI 0.07-0.48; P=0.001) although confounding with NHL was apparent. Our data emphasise the risk of PTLD associated with alemtuzumab. Furthermore, we report the clinically important observation that rituximab, administered in the peri-transplant period, may provide effective prophylaxis for PTLD.
EB病毒相关的移植后淋巴细胞增殖性疾病(PTLD)仍然是异基因造血干细胞移植(allo-HSCT)的一个重要并发症。我们回顾性分析了在单一中心接受连续异基因造血干细胞移植并使用阿仑单抗进行T细胞清除的186例成年患者中EB病毒再激活的发生率和危险因素。到1年时,EB病毒再激活的累积发生率为48%(置信区间(CI)41-55%),高水平EB病毒再激活的发生率为18%(CI 13-24%);8例患者同时被诊断为PTLD。在高水平再激活的患者中,31/38(82%)在首次EB病毒定量聚合酶链反应(qPCR)阳性后的2周内就出现了这种情况。单因素分析显示,年龄≥50岁与EB病毒再激活风险显著增加相关(风险比(HR)1.54,CI 1.02-2.31;P=0.039)。此外,非霍奇金淋巴瘤(NHL)的诊断与再激活风险大幅降低相关(HR 0.10,CI 0.03-0.33;P=0.0001),这在多因素检测中得到了证实。重要的是,异基因造血干细胞移植前6个月内使用利妥昔单抗治疗也高度预示不会发生EB病毒再激活(HR 0.18,CI 0.07-0.48;P=0.001),尽管与NHL存在明显的混杂因素。我们的数据强调了与阿仑单抗相关的PTLD风险。此外,我们报告了一个具有临床重要性的观察结果,即在移植围手术期使用利妥昔单抗可能为PTLD提供有效的预防。