Krishnamoorthi Rajesh, Singh Siddharth, Ragunathan Karthik, A Katzka David, K Wang Kenneth, G Iyer Prasad
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Mayo Clinic, Rochester, Minnesota, USA.
Department of Internal Medicine, University of Illinois College of Medicine, Peoria, Illinois, USA.
Gastrointest Endosc. 2016 Jun;83(6):1090-1106.e3. doi: 10.1016/j.gie.2016.02.009. Epub 2016 Feb 20.
Previous estimates of incidence of intestinal metaplasia (IM) recurrence after achieving complete remission of IM (CRIM) through endoscopic therapy of Barrett's esophagus (BE) have varied widely. We performed a systematic review and meta-analysis of studies to estimate an accurate recurrence risk after CRIM.
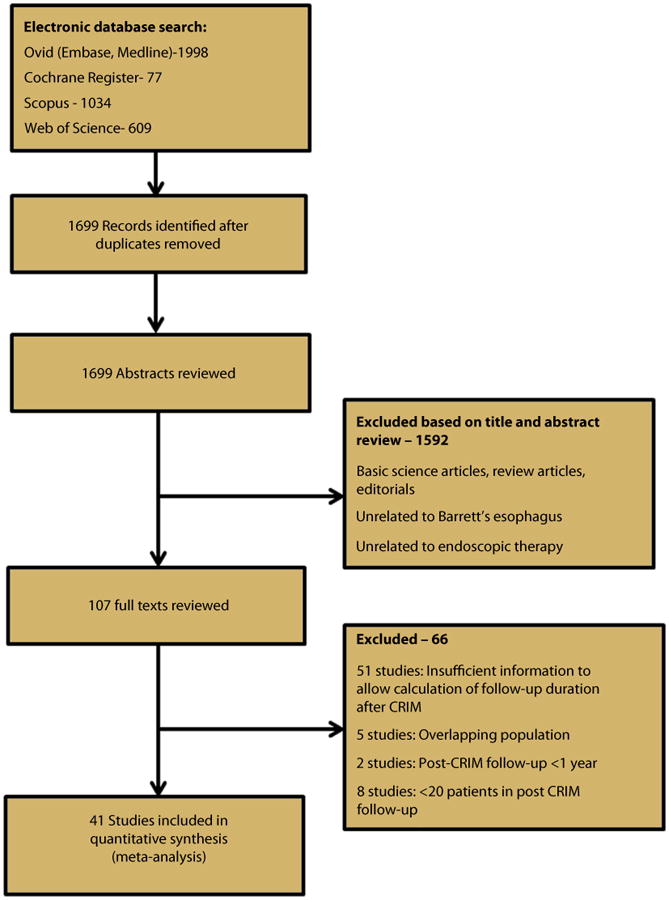
We performed a systematic search of multiple literature databases through June 2015 to identify studies reporting long-term follow-up after achieving CRIM through endoscopic therapy. Pooled incidence rate (IR) of recurrent IM, dysplastic BE, and high-grade dysplasia (HGD)/esophageal adenocarcinoma (EAC) per person-year of follow-up after CRIM was estimated. Factors associated with recurrence were also assessed.
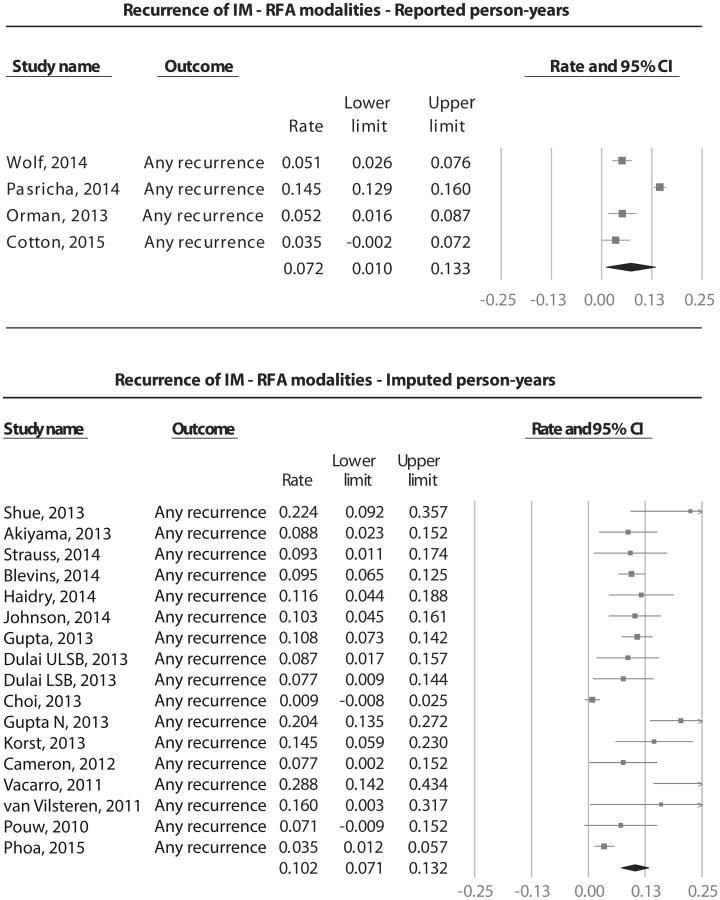
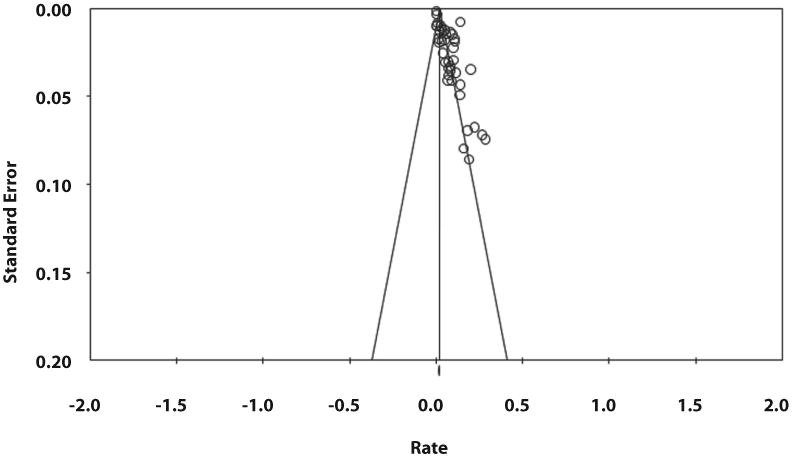
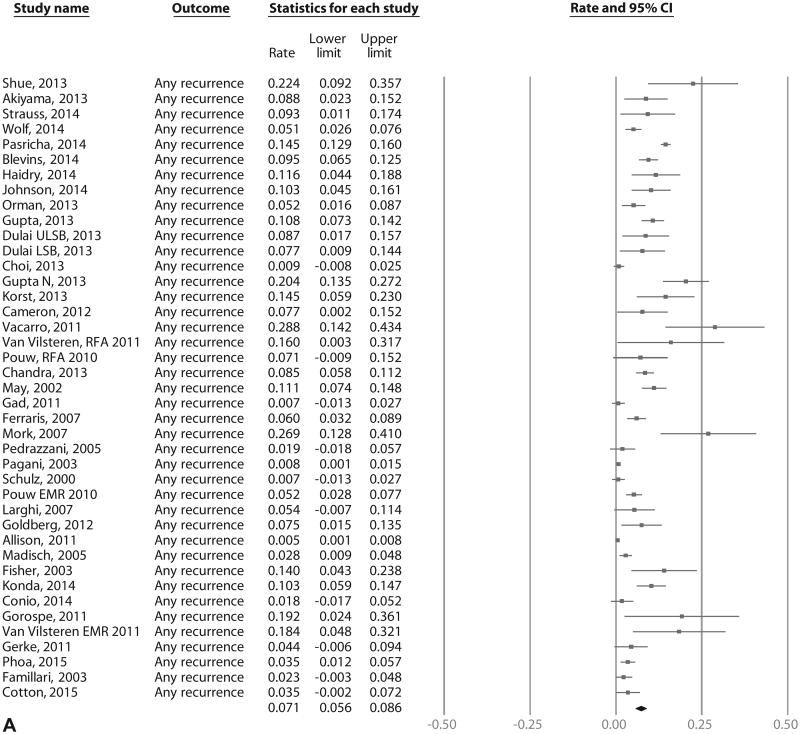
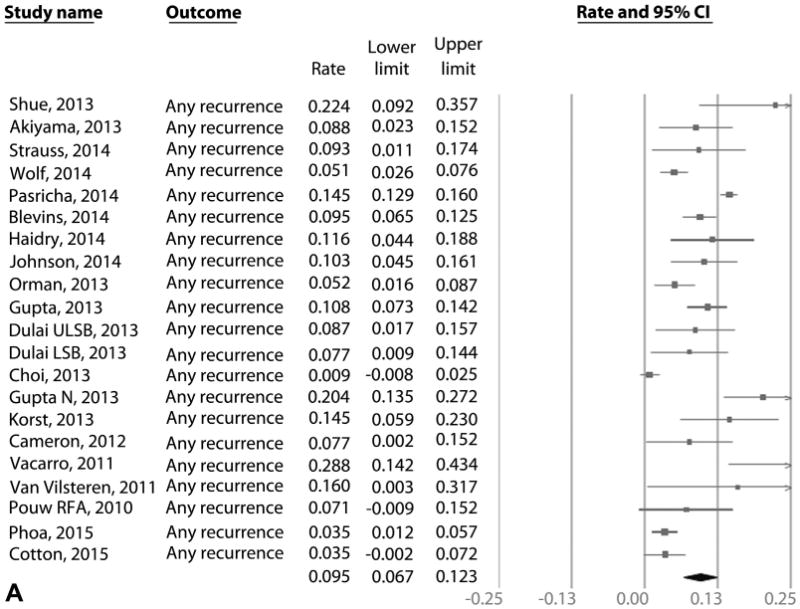
We identified 41 studies that reported 795 cases of recurrence in 4443 patients over 10,427 patient-years of follow-up. This included 21 radiofrequency ablation studies that reported 603 cases of IM recurrence in 3186 patients over 5741 patient-years of follow-up. Pooled IRs of recurrent IM, dysplastic BE, and HGD/EAC after radiofrequency ablation were 9.5% (95% CI, 6.7-12.3), 2.0% (95% CI, 1.3-2.7), and 1.2% (95% CI, .8-1.6) per patient-year, respectively. When all endoscopic modalities were included, pooled IRs of recurrent IM, dysplastic BE, and HGD/EAC were 7.1% (95% CI, 5.6-8.6), 1.3% (95% CI, .8-1.7), and .8% (95% CI, .5-1.1) per patient-year, respectively. Substantial heterogeneity was noted. Increasing age and BE length were predictive of recurrence; 97% of recurrences were treated endoscopically.
The incidence of recurrence after achieving CRIM through endoscopic therapy was substantial. A small minority of recurrences were dysplastic BE and HGD/EAC. Hence, continued surveillance after CRIM is imperative. Additional studies with long-term follow-up are needed.
既往关于通过内镜治疗巴雷特食管(BE)实现肠化生(IM)完全缓解(CRIM)后IM复发率的估计差异很大。我们对相关研究进行了系统评价和荟萃分析,以估计CRIM后的准确复发风险。
我们对多个文献数据库进行了系统检索,截至2015年6月,以确定报告通过内镜治疗实现CRIM后的长期随访情况的研究。估计了CRIM后每人每年复发性IM、发育异常BE和高级别发育异常(HGD)/食管腺癌(EAC)的合并发病率(IR)。还评估了与复发相关的因素。
我们确定了41项研究,在10427患者年的随访中,报告了4443例患者中有795例复发。其中包括21项射频消融研究,在5741患者年的随访中,报告了3186例患者中有603例IM复发。射频消融后复发性IM、发育异常BE和HGD/EAC的合并IR分别为每人每年9.5%(95%CI,6.7-12.3)、2.0%(95%CI,1.3-2.7)和1.2%(95%CI,0.8-1.6)。当纳入所有内镜治疗方式时,复发性IM、发育异常BE和HGD/EAC的合并IR分别为每人每年7.1%(95%CI,5.6-8.6)、1.3%(95%CI,0.8-1.7)和0.8%(95%CI,0.5-1.1)。观察到显著的异质性。年龄增加和BE长度增加是复发的预测因素;97%的复发通过内镜治疗。
通过内镜治疗实现CRIM后的复发率较高。少数复发为发育异常BE和HGD/EAC。因此,CRIM后持续监测至关重要。需要更多长期随访的研究。