Bitker Laurent, Bayle Frédérique, Yonis Hodane, Gobert Florent, Leray Véronique, Taponnier Romain, Debord Sophie, Stoian-Cividjian Alina, Guérin Claude, Richard Jean-Christophe
Service de Réanimation Médicale, Hôpital De La Croix Rousse, Hospices Civils de Lyon, 103 Grande Rue de la Croix Rousse, 69004, Lyon, France.
Faculté de médecine Lyon-Est, Université de Lyon, Université Lyon I, 92 Rue Pasteur, 69007, Lyon, France.
Crit Care. 2016 Feb 23;20:44. doi: 10.1186/s13054-016-1227-3.
Hypotension is a frequent complication of intermittent hemodialysis (IHD) performed in intensive care units (ICUs). Passive leg raising (PLR) combined with continuous measurement of cardiac output is highly reliable to identify preload dependence, and may provide new insights into the mechanisms involved in IHD-related hypotension. The aim of this study was to assess prevalence and risk factors of preload dependence-related hypotension during IHD in the ICU.
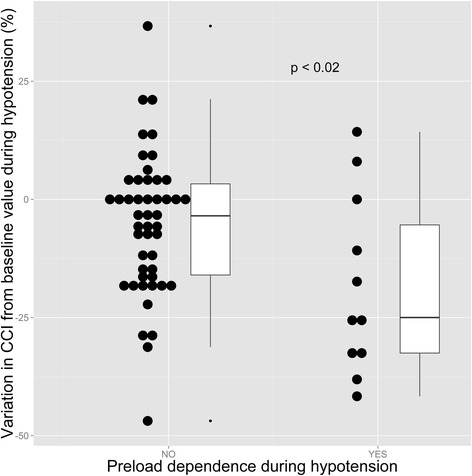
A single-center prospective observational study performed on ICU patients undergoing IHD for acute kidney injury and monitored with a PiCCO® device. Primary end points were the prevalence of hypotension (defined as a mean arterial pressure below 65 mm Hg) and hypotension associated with preload dependence. Preload dependence was assessed by the passive leg raising test, and considered present if the systolic ejection volume increased by at least 10% during the test, as assessed continuously by the PiCCO® device.
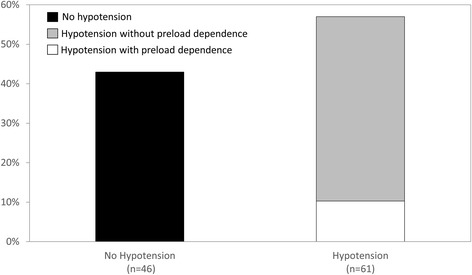
Forty-seven patients totaling 107 IHD sessions were included. Hypotension was observed in 61 IHD sessions (57%, CI95%: 47-66%) and was independently associated with inotrope administration, higher SOFA score, lower time lag between ICU admission and IHD session, and lower MAP at IHD session onset. Hypotension associated with preload dependence was observed in 19% (CI95%: 10-31%) of sessions with hypotension, and was associated with mechanical ventilation, lower SAPS II, higher pulmonary vascular permeability index (PVPI) and dialysate sodium concentration at IHD session onset. ROC curve analysis identified PVPI and mechanical ventilation as the only variables with significant diagnostic performance to predict hypotension associated with preload dependence (respective AUC: 0.68 (CI95%: 0.53-0.83) and 0.69 (CI95%: 0.54-0.85). A PVPI ≥ 1.6 at IHD session onset predicted occurrence of hypotension associated with preload dependence during IHD with a sensitivity of 91% (CI95%: 59-100%), and a specificity of 53% (CI95%: 42-63%).
The majority of hypotensive episodes occurring during intermittent hemodialysis are unrelated to preload dependence and should not necessarily lead to reduction of fluid removal by hemodialysis. However, high PVPI at IHD session onset and mechanical ventilation are risk factors of preload dependence-related hypotension, and should prompt reduction of planned fluid removal during the session, and/or an increase in session duration.
低血压是重症监护病房(ICU)进行间歇性血液透析(IHD)时常见的并发症。被动抬腿(PLR)联合连续测量心输出量对于识别前负荷依赖性非常可靠,并且可能为IHD相关低血压的发病机制提供新的见解。本研究的目的是评估ICU中IHD期间前负荷依赖性相关低血压的患病率和危险因素。
对因急性肾损伤接受IHD并使用脉波指示剂连续心输出量监测仪(PiCCO®)进行监测的ICU患者进行单中心前瞻性观察研究。主要终点是低血压(定义为平均动脉压低于65mmHg)的患病率以及与前负荷依赖性相关的低血压。通过被动抬腿试验评估前负荷依赖性,如果在试验期间收缩期射血容积增加至少10%(由PiCCO®设备连续评估),则认为存在前负荷依赖性。
共纳入47例患者,总计107次IHD治疗。在61次IHD治疗中观察到低血压(57%,95%CI:47-66%),且与使用血管活性药物、较高的序贯器官衰竭评估(SOFA)评分、ICU入院至IHD治疗的时间间隔较短以及IHD治疗开始时较低的平均动脉压独立相关。在发生低血压的治疗中,19%(95%CI:10-31%)观察到与前负荷依赖性相关的低血压,且与机械通气、较低的简化急性生理学评分II(SAPS II)、较高的肺血管通透性指数(PVPI)以及IHD治疗开始时的透析液钠浓度相关。受试者工作特征(ROC)曲线分析确定PVPI和机械通气是预测与前负荷依赖性相关低血压具有显著诊断性能的唯一变量(各自的曲线下面积[AUC]:0.68[95%CI:0.53-0.83]和0.69[95%CI:0.54-0.85])。IHD治疗开始时PVPI≥1.6预测IHD期间与前负荷依赖性相关低血压的发生,敏感性为91%(95%CI:59-100%),特异性为53%(95%CI:42-63%)。
间歇性血液透析期间发生的大多数低血压发作与前负荷依赖性无关,不一定会导致血液透析液体清除量的减少。然而,IHD治疗开始时较高的PVPI和机械通气是前负荷依赖性相关低血压的危险因素,应促使在治疗期间减少计划的液体清除量和/或增加治疗持续时间。