Alonso Alvaro, Roetker Nicholas S, Soliman Elsayed Z, Chen Lin Y, Greenland Philip, Heckbert Susan R
Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN
Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN.
J Am Heart Assoc. 2016 Feb 23;5(2):e003077. doi: 10.1161/JAHA.115.003077.
Existing equations for prediction of atrial fibrillation (AF) have been developed and validated in white and African-American populations. Whether these models adequately predict AF in more racially and ethnically diverse populations is unknown.
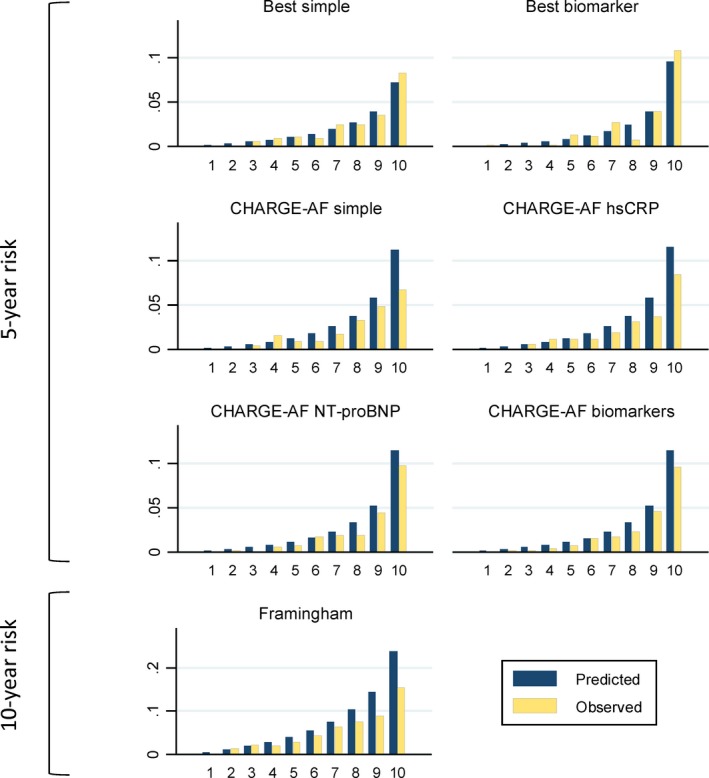
We studied 6663 men and women 45 to 84 years of age without AF at baseline (2000-2002) enrolled in the Multi-Ethnic Study of Atherosclerosis (MESA). Of these, 38% were non-Hispanic whites, 28% non-Hispanic African Americans, 22% Hispanics, and 12% Chinese Americans. AF during follow-up was ascertained from hospitalization discharge codes through 2012. Information collected at baseline was used to calculate predicted 5-year risk of AF using the previously published simple CHARGE-AF model, which only includes clinical variables, and a biomarker-enriched CHARGE-AF model, which also considers levels of circulating N-terminal of the prohormone B-type natriuretic peptide and C-reactive protein. For comparison purposes, we also assessed performance of the 10-year Framingham AF model. During a mean follow-up of 10.2 years, 351 cases of AF were identified. The C-statistic of the CHARGE-AF models were 0.779 (95% CI, 0.744-0.814) for the simple model and 0.825 (95% CI, 0.791-0.860) for the biomarker-enriched model. Calibration was adequate in the biomarker-enriched model (χ(2)=7.9; P=0.55), but suboptimal in the simple model (χ(2)=25.6; P=0.002). In contrast, the 10-year Framingham score had a C-statistic (95% CI) of 0.746 (0.720-0.771) and showed poor calibration (χ(2)=57.4; P<0.0001).
The CHARGE-AF risk models adequately predicted 5-year AF risk in a large multiethnic cohort. These models could be useful to select high-risk individuals for AF screening programs or for primary prevention trials in diverse populations.
现有的预测心房颤动(AF)的方程是在白人和非裔美国人人群中开发并验证的。这些模型在种族和民族更加多样化的人群中能否充分预测AF尚不清楚。
我们研究了参加动脉粥样硬化多民族研究(MESA)的6663名45至84岁、基线时(2000 - 2002年)无AF的男性和女性。其中,38%为非西班牙裔白人,28%为非西班牙裔非裔美国人,22%为西班牙裔,12%为华裔美国人。通过2012年的住院出院编码确定随访期间的AF情况。使用先前发表的仅包括临床变量的简单CHARGE - AF模型以及还考虑循环前激素B型利钠肽N端和C反应蛋白水平的富含生物标志物的CHARGE - AF模型,利用基线收集的信息计算预测的5年AF风险。为作比较,我们还评估了10年弗雷明汉AF模型的性能。在平均10.2年的随访期间,共识别出351例AF病例。简单模型的CHARGE - AF模型的C统计量为0.779(95%CI,0.744 - 0.814),富含生物标志物的模型为0.825(95%CI,0.791 - 0.860)。富含生物标志物的模型校准良好(χ(2)=7.9;P = 0.55),而简单模型校准欠佳(χ(2)=25.6;P = 0.002)。相比之下,10年弗雷明汉评分的C统计量(95%CI)为0.746(0.720 - 0.771),校准较差(χ(2)=57.4;P < 0.0001)。
CHARGE - AF风险模型在一个大型多民族队列中充分预测了5年AF风险。这些模型可能有助于为AF筛查项目或不同人群的一级预防试验选择高危个体。