Hitchings Andrew W, Lai Dilys, Jones Paul W, Baker Emma H
Institute for Infection and Immunity, St George's, University of London, London, UK.
Chelsea and Westminster Hospital NHS Foundation Trust, London, UK.
Thorax. 2016 Jul;71(7):587-93. doi: 10.1136/thoraxjnl-2015-208035. Epub 2016 Feb 25.
Severe exacerbations of COPD are commonly associated with hyperglycaemia, which predicts adverse outcomes. Metformin is a well-established anti-hyperglycaemic agent in diabetes mellitus, possibly augmented with anti-inflammatory effects, but its effects in COPD are unknown. We investigated accelerated metformin therapy in severe COPD exacerbations, primarily to confirm or refute an anti-hyperglycaemic effect, and secondarily to explore its effects on inflammation and clinical outcome.
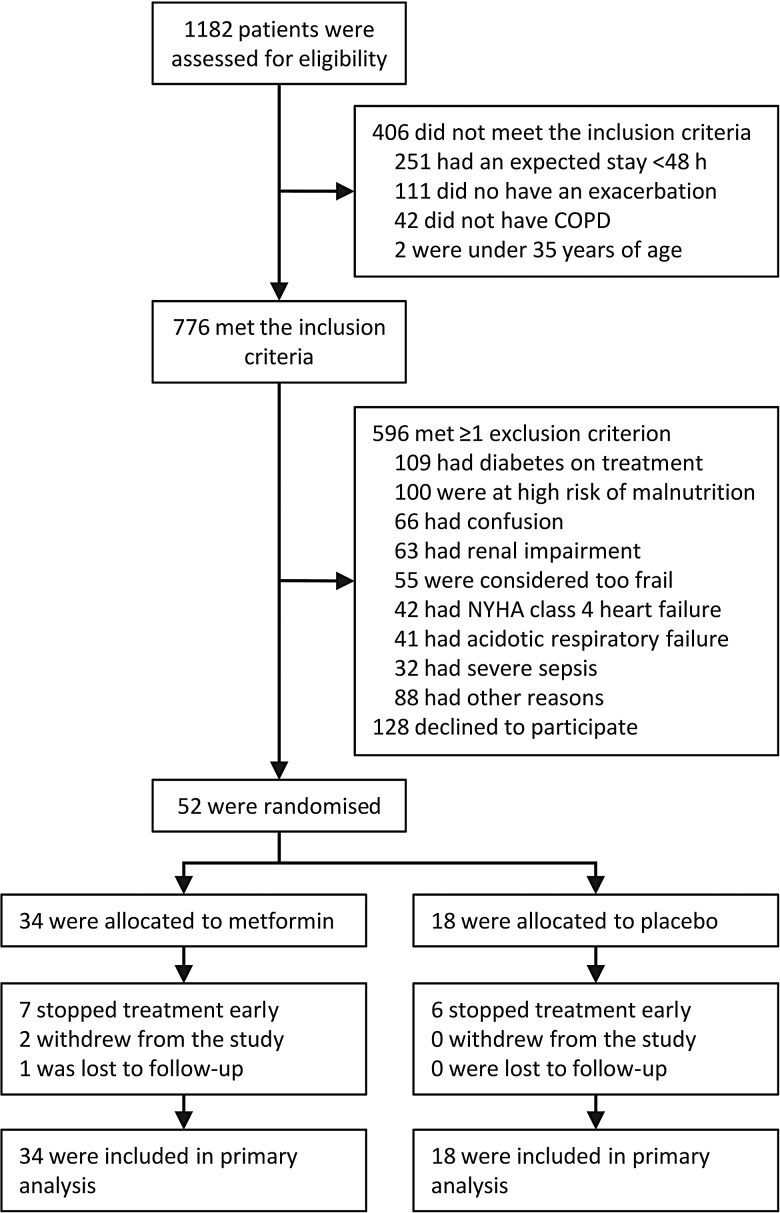
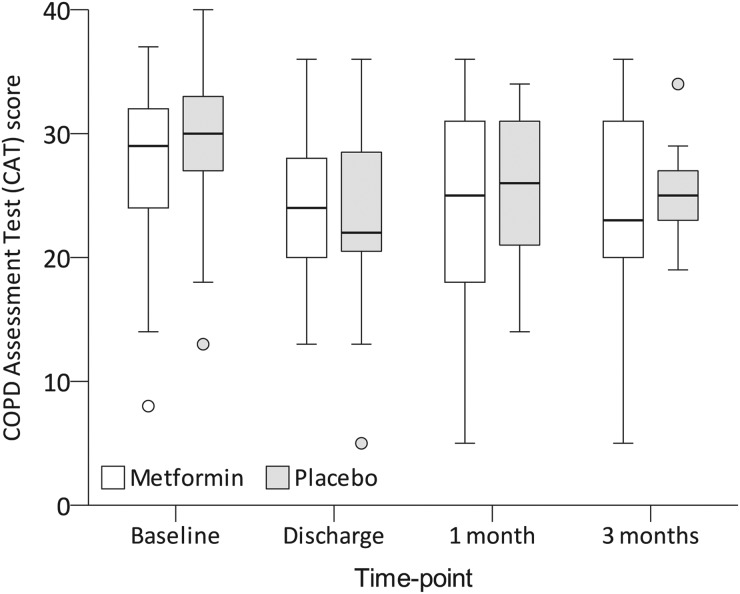
This was a multicentre, randomised, double-blind, placebo-controlled trial testing accelerated metformin therapy in non-diabetic patients, aged ≥35 years, hospitalised for COPD exacerbations. Participants were assigned in a 2:1 ratio to 1 month of metformin therapy, escalated rapidly to 2 g/day, or matched placebo. The primary end point was mean in-hospital blood glucose concentration. Secondary end points included the concentrations of fructosamine and C reactive protein (CRP), and scores on the COPD Assessment Test and Exacerbations of Chronic Pulmonary Disease Tool.
52 participants (mean (±SD) age 67±9 years) were randomised (34 to metformin, 18 to placebo). All were included in the primary end point analysis. The mean blood glucose concentrations in the metformin and placebo groups were 7.1±0.9 and 8.0±3.3 mmol/L, respectively (difference -0.9 mmol/L, 95% CI -2.1 to +0.3; p=0.273). No significant between-group differences were observed on any of the secondary end points. Adverse reactions, particularly gastrointestinal effects, were more common in metformin-treated participants.
Metformin did not ameliorate elevations in blood glucose concentration among non-diabetic patients admitted to hospital for COPD exacerbations, and had no detectable effect on CRP or clinical outcomes.
ISRCTN66148745 and NCT01247870.
慢性阻塞性肺疾病(COPD)的严重加重通常与高血糖相关,高血糖可预测不良结局。二甲双胍是糖尿病中一种成熟的抗高血糖药物,可能具有抗炎作用增强,但它在COPD中的作用尚不清楚。我们研究了在严重COPD加重期加速使用二甲双胍治疗,主要是为了证实或反驳其抗高血糖作用,其次是探索其对炎症和临床结局的影响。
这是一项多中心、随机、双盲、安慰剂对照试验,对年龄≥35岁、因COPD加重而住院的非糖尿病患者进行加速二甲双胍治疗试验。参与者按2:1的比例分配,接受为期1个月的二甲双胍治疗,迅速递增至2克/天,或匹配的安慰剂。主要终点是住院期间的平均血糖浓度。次要终点包括果糖胺和C反应蛋白(CRP)浓度,以及COPD评估测试和慢性肺病加重工具的评分。
52名参与者(平均(±标准差)年龄67±9岁)被随机分组(34名接受二甲双胍治疗,18名接受安慰剂治疗)。所有参与者均纳入主要终点分析。二甲双胍组和安慰剂组的平均血糖浓度分别为7.1±0.9和8.0±3.3毫摩尔/升(差异-0.9毫摩尔/升,95%置信区间-2.1至+0.3;p=0.273)。在任何次要终点上均未观察到显著的组间差异。不良反应,尤其是胃肠道效应,在接受二甲双胍治疗的参与者中更为常见。
对于因COPD加重而住院的非糖尿病患者,二甲双胍并不能改善血糖浓度升高,对CRP或临床结局也没有可检测到的影响。
ISRCTN66148745和NCT01247870。