Thurston Rebecca C, Matthews Karen A, Chang Yuefang, Santoro Nanette, Barinas-Mitchell Emma, von Känel Roland, Landsittel Doug P, Jennings J Richard
1Department of Psychiatry, University of Pittsburgh School of Medicine, Pittsburgh, PA 2Department of Epidemiology, University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA 3Department of Neurosurgery, University of Pittsburgh School of Medicine, Pittsburgh, PA 4Department of Obstetrics and Gynecology, University of Colorado School of Medicine, Denver, CO 5Department of Neurology, Inselspital, Bern University Hospital, and University of Bern, Switzerland 6Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA.
Menopause. 2016 May;23(5):499-505. doi: 10.1097/GME.0000000000000586.
Most midlife women report vasomotor symptoms (VMS), yet their physiology remains poorly understood. This study tested whether acute decreases in cardiac vagal control would occur with VMS in a large sample of women monitored during wake and sleep.
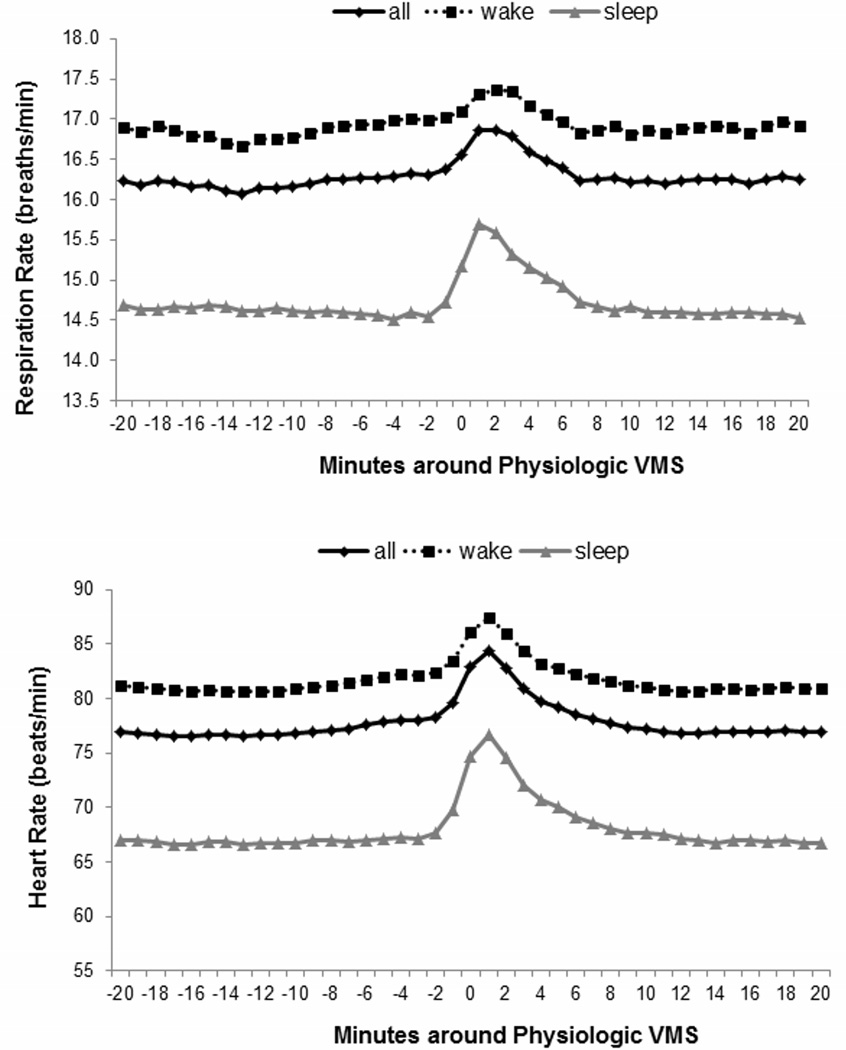
Two hundred and fifteen nonsmoking women aged 40 to 60 years with evidence of VMS were included. Women were free of a history of clinical cardiovascular disease or arrhythmia; or use of insulin, beta blockers, calcium channel blockers, or medications impacting VMS. Women underwent 24 hours of ambulatory monitoring for physiological (sternal skin conductance) and self-report (electronic diary) measurement of VMS; heart rate variability (electrocardiogram); and respiratory rate. Changes in cardiac vagal control as assessed by respiratory sinus arrhythmia during VMS, relative to periods before and after VMS, were tested in linear mixed models.
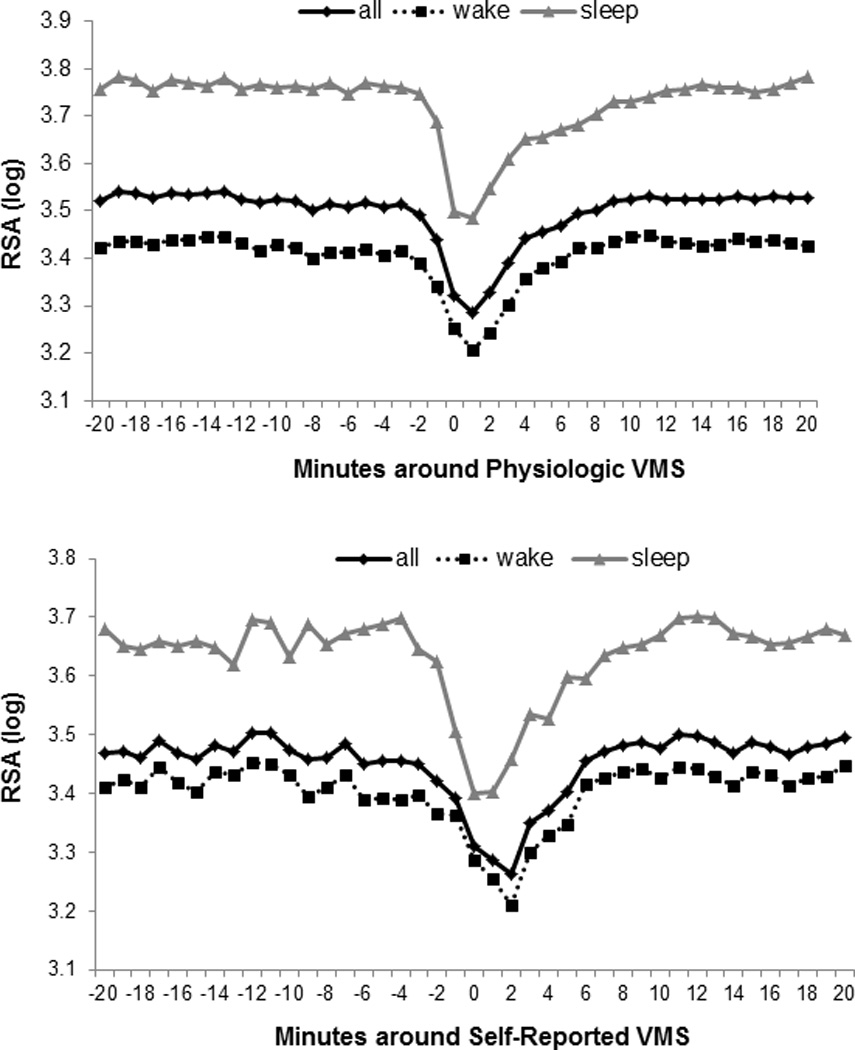
Significant decreases in respiratory sinus arrhythmia were observed during physiologically measured VMS relative to periods preceding (b[SE] = 0.13 (0.004), P < 0.0001) and after the vasomotor symptoms (b[SE] = 0.13 (0.004), P < 0.0001), adjusted for age, race, body mass index, and sleep/wake status. Decreases were observed for women not aware of their VMS, and differences persisted controlling for respiration rate. Interactions indicated that respiratory sinus arrhythmia decreases were most pronounced during sleep and for younger women.
Physiologically measured VMS were accompanied by an inhibition of cardiac vagal control in a large sample of women. Changes were observed irrespective of whether the VMS were reported, were most pronounced during sleep, and were greatest among younger women. These findings contribute to the understanding of vasomotor symptom physiology.
大多数中年女性报告有血管舒缩症状(VMS),但其生理机制仍知之甚少。本研究在大量清醒和睡眠期间接受监测的女性样本中,测试血管舒缩症状发作时心脏迷走神经控制是否会急性下降。
纳入215名年龄在40至60岁之间、有血管舒缩症状证据的非吸烟女性。这些女性无临床心血管疾病或心律失常病史;未使用胰岛素、β受体阻滞剂、钙通道阻滞剂或影响血管舒缩症状的药物。女性接受24小时动态监测,以进行血管舒缩症状的生理测量(胸骨皮肤电导)和自我报告(电子日记);心率变异性(心电图);以及呼吸频率。在线性混合模型中测试血管舒缩症状发作期间通过呼吸性窦性心律不齐评估的心脏迷走神经控制变化,相对于血管舒缩症状发作之前和之后的时间段。
在生理测量的血管舒缩症状发作期间,相对于发作前(b[标准误]=0.13(0.004),P<0.0001)和血管舒缩症状发作后(b[标准误]=0.13(0.004),P<0.0001),观察到呼吸性窦性心律不齐显著下降,校正了年龄、种族、体重指数和睡眠/觉醒状态。未意识到自己有血管舒缩症状的女性也观察到下降,且在控制呼吸频率后差异仍然存在。交互作用表明,呼吸性窦性心律不齐的下降在睡眠期间和年轻女性中最为明显。
在大量女性样本中,生理测量的血管舒缩症状伴有心脏迷走神经控制的抑制。无论是否报告血管舒缩症状,均观察到变化,在睡眠期间最为明显,在年轻女性中最大。这些发现有助于理解血管舒缩症状的生理机制。