Travassos Mark A, Beyene Berhane, Adam Zenaw, Campbell James D, Mulholland Nigisti, Diarra Seydou S, Kassa Tassew, Oot Lisa, Sequeira Jenny, Reymann Mardi, Blackwelder William C, Wu Yukun, Ruslanova Inna, Goswami Jaya, Sow Samba O, Pasetti Marcela F, Steinglass Robert, Kebede Amha, Levine Myron M
Center for Vaccine Development, University of Maryland School of Medicine, Baltimore, Maryland, United States of America.
Ethiopian Public Health Institute, Addis Ababa, Ethiopia.
PLoS One. 2016 Mar 2;11(3):e0149970. doi: 10.1371/journal.pone.0149970. eCollection 2016.
Demographic and health surveys, immunization coverage surveys and administrative data often divergently estimate vaccination coverage, which hinders pinpointing districts where immunization services require strengthening. We assayed vaccination coverage in three regions in Ethiopia by coverage surveys and linked serosurveys.
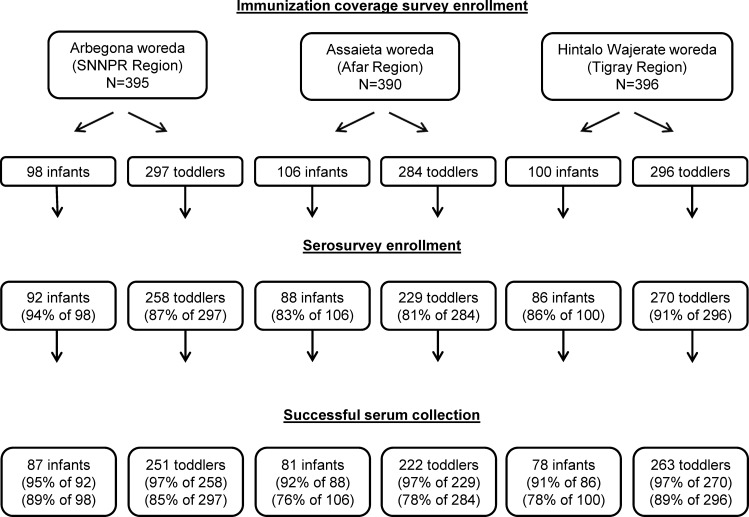
Households with children aged 12-23 (N = 300) or 6-8 months (N = 100) in each of three districts (woredas) were randomly selected for immunization coverage surveys (inspection of vaccination cards and immunization clinic records and maternal recall) and linked serosurveys. IgG-ELISA serologic biomarkers included tetanus antitoxin ≥ 0.15 IU/ml in toddlers (receipt of tetanus toxoid) and Haemophilus influenzae type b (Hib) anti-capsular titers ≥ 1.0 mcg/ml in infants (timely receipt of Hib vaccine).
Coverage surveys enrolled 1,181 children across three woredas; 1,023 (87%) also enrolled in linked serosurveys. Administrative data over-estimated coverage compared to surveys, while maternal recall was unreliable. Serologic biomarkers documented a hierarchy among the districts. Biomarker measurement in infants provided insight on timeliness of vaccination not deducible from toddler results.
Neither administrative projections, vaccination card or EPI register inspections, nor parental recall, substitute for objective serological biomarker measurement. Including infants in serosurveys informs on vaccination timeliness.
人口与健康调查、免疫接种覆盖率调查及行政数据对疫苗接种覆盖率的估算往往存在差异,这妨碍了确定哪些地区的免疫服务需要加强。我们通过覆盖率调查和相关血清学调查对埃塞俄比亚三个地区的疫苗接种覆盖率进行了测定。
在三个区(沃雷达斯)中,每个区随机选择有12至23个月大儿童(N = 300)或6至8个月大儿童(N = 100)的家庭进行免疫接种覆盖率调查(检查疫苗接种卡、免疫接种诊所记录及母亲回忆)和相关血清学调查。IgG-ELISA血清学生物标志物包括幼儿破伤风抗毒素≥0.15 IU/ml(接种破伤风类毒素)及婴儿b型流感嗜血杆菌(Hib)抗荚膜滴度≥1.0 mcg/ml(及时接种Hib疫苗)。
覆盖率调查在三个沃雷达斯共纳入1181名儿童;其中1023名(87%)也纳入了相关血清学调查。与调查结果相比,行政数据高估了覆盖率,而母亲回忆不可靠。血清学生物标志物显示了各区之间的层级关系。婴儿生物标志物测量提供了从幼儿结果中无法推断出的疫苗接种及时性的见解。
行政预测、疫苗接种卡或扩大免疫规划登记检查以及家长回忆均不能替代客观的血清学生物标志物测量。血清学调查纳入婴儿有助于了解疫苗接种的及时性。