Warusevitane Anushka, Karunatilake Dumin, Sim Julius, Smith Craig, Roffe Christine
Stoke Stroke Research Group, University Hospitals of North Midlands, Stoke-on-Trent, United Kingdom.
Stroke Unit, Taunton and Somerset NHS Trust, Taunton, United Kingdom.
PLoS One. 2016 Mar 3;11(3):e0150269. doi: 10.1371/journal.pone.0150269. eCollection 2016.
Accurate diagnosis of pneumonia complicating severe stroke is challenging due to difficulties in physical examination, altered immune responses and delayed manifestations of radiological changes. The aims of this study were to describe early clinical features and to examine C-reactive protein (CRP) as a diagnostic marker of post-stroke pneumonia.
Patients who required nasogastric feeding and had no evidence of pneumonia within 7 days of stroke onset were included in the study and followed-up for 21 days with a daily clinical examination. Pneumonia was diagnosed using modified British Thoracic Society criteria.
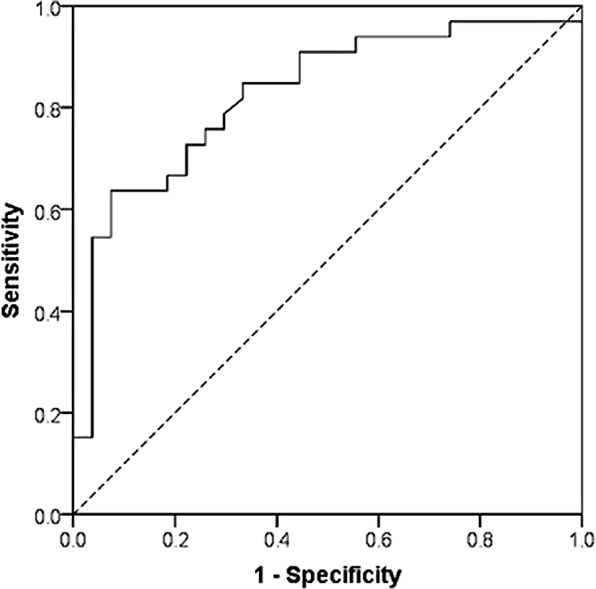
60 patients were recruited (mean age 77 years, mean National Institutes of Health Stroke Scale Score 19.47). Forty-four episodes of pneumonia were identified. Common manifestations on the day of the diagnosis were new onset crackles (43/44, 98%), tachypnoea>25/min (42/44, 95%), and oxygen saturation <90% (41/44, 93%). Cough, purulent sputum, and pyrexia >38°C were observed in 27 (61%), 25 (57%) and 15 (34%) episodes respectively. Leucocytosis (WBC>11,000/ml) and raised CRP (>10 mg/l) were observed in 38 (86%) and 43 (97%) cases of pneumonia respectively. The area under the ROC curve for CRP was 0.827 (95% CI 0.720, 0.933). The diagnostic cut-off for CRP with an acceptable sensitivity (>0.8) was 25.60 mg/L (Youden index (J) 0.515; sensitivity 0.848; specificity 0.667). A cut-off of 64.65 mg/L had the highest diagnostic accuracy (J 0.562; sensitivity 0.636; specificity 0.926).
Patients with severe stroke frequently do not manifest key diagnostic features of pneumonia such as pyrexia, cough and purulent sputum early in their illness. The most common signs in this group are new-onset crackles, tachypnoea and hypoxia. Our results suggest that a CRP >25 mg/L should prompt investigations for pneumonia while values >65 mg/L have the highest diagnostic accuracy to justify consideration of this threshold as a diagnostic marker of post-stroke pneumonia.
由于体格检查困难、免疫反应改变以及放射学变化出现延迟,准确诊断重症卒中合并肺炎具有挑战性。本研究的目的是描述早期临床特征,并检验C反应蛋白(CRP)作为卒中后肺炎的诊断标志物。
纳入需要鼻饲且在卒中发作7天内无肺炎证据的患者,进行为期21天的每日临床检查随访。采用改良的英国胸科学会标准诊断肺炎。
共招募60例患者(平均年龄77岁,美国国立卫生研究院卒中量表平均评分19.47)。确定了44例肺炎发作。诊断当天的常见表现为新发啰音(43/44,98%)、呼吸急促>25次/分钟(42/44,95%)以及氧饱和度<90%(41/44,93%)。分别在27例(61%)、25例(57%)和15例(34%)发作中观察到咳嗽、脓性痰和发热>38°C。肺炎患者中分别有38例(86%)和43例(97%)出现白细胞增多(白细胞>11,000/ml)和CRP升高(>10mg/l)。CRP的ROC曲线下面积为0.827(95%CI 0.720,0.933)。具有可接受敏感性(>0.8)的CRP诊断临界值为25.60mg/L(约登指数(J)0.515;敏感性0.848;特异性0.667)。临界值为64.65mg/L时诊断准确性最高(J 0.562;敏感性0.636;特异性0.926)。
重症卒中患者在疾病早期常未表现出肺炎的关键诊断特征,如发热、咳嗽和脓性痰。该组最常见的体征是新发啰音、呼吸急促和缺氧。我们的结果表明,CRP>25mg/L应促使对肺炎进行检查,而>65mg/L的值诊断准确性最高,有理由将该阈值视为卒中后肺炎的诊断标志物。