Ellington David Rich, Szychowski Jeffery Michael, Malek Joseph Michael, Gerten Kimberly Anne, Burgio Kathryn Larsen, Richter Holly Elizabeth
From the *Division of Urogynecology and Pelvic Reconstructive Surgery, Department of Obstetrics and Gynecology, and †Department of Biostatistics, University of Alabama at Birmingham, Birmingham, AL; ‡Urogynecology and Reconstructive Pelvic Surgery, Park Nicollet Health, St Louis Park, MN; and §Department of Medicine, University of Alabama at Birmingham; and Birmingham/Atlanta Geriatric Research, Education, and Clinical Center, Department of Veterans Affairs, Birmingham, AL.
Female Pelvic Med Reconstr Surg. 2016 Jul-Aug;22(4):254-60. doi: 10.1097/SPV.0000000000000256.
The aims of this study were to compare 12-week outcomes of single-therapy tolterodine (Detrol LA) extended release to intravaginal estrogen (Estrace) for overactive bladder (OAB) symptoms and characterize 24- and 52-week outcomes in women undergoing combined therapy.
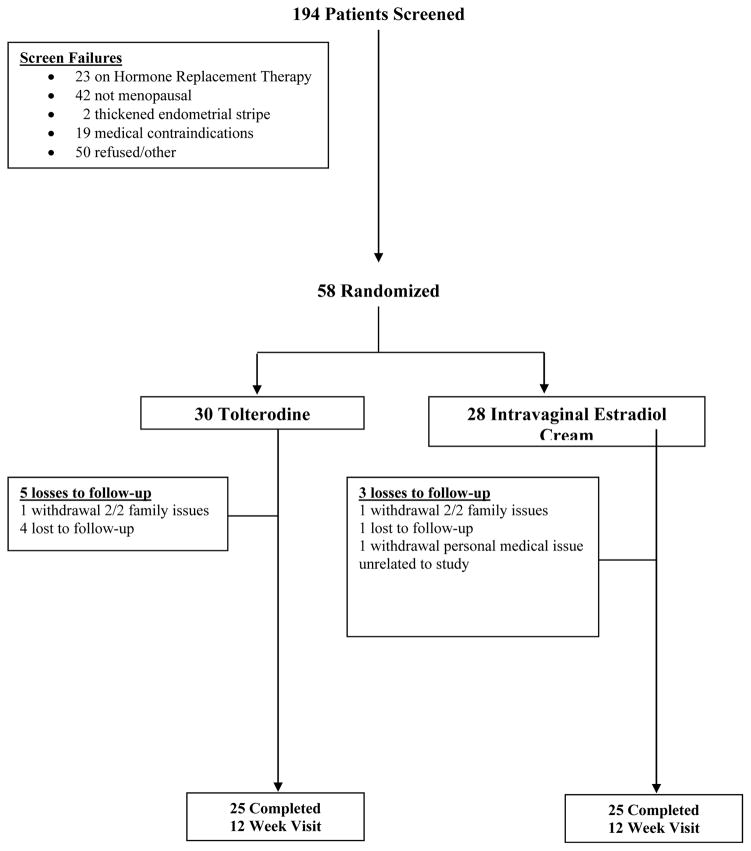
A single-site randomized, open-label trial in women with urinary frequency, urgency, nocturia, and/or urgency urinary incontinence symptoms was performed. Fifty-eight participants were randomized to oral tolterodine extended release daily or intravaginal estradiol cream nightly for 6 weeks then twice per week. The primary outcome was change in Overactive Bladder Questionnaire (OAB-q) symptom bother score at 12 weeks. Secondary outcomes included the Health-Related Quality of Life Questionnaire (HRQL) of the OAB-q and a 3-day bladder diary. At 12 weeks, subjects were offered addition of the alternative therapy with follow-up at 24 and 52 weeks.
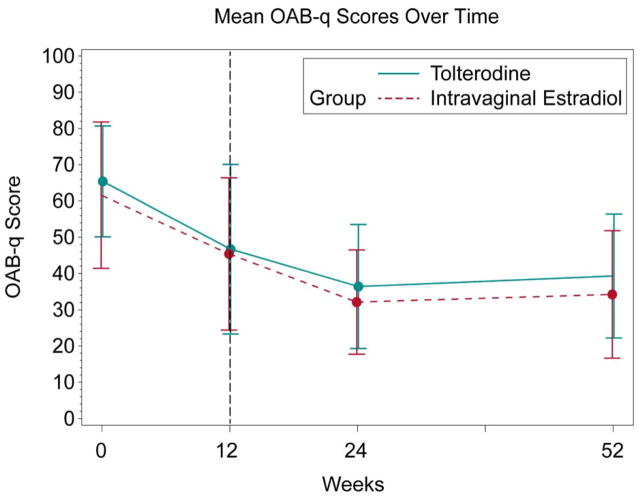
There was no difference in symptom bother score improvement between the tolterodine and intravaginal estradiol groups baseline to 12 weeks (20.6 ± 21.7, -15.8 ± 23.3, respectively, P = 0.45). There was a significant within-group decrease in symptom bother score from baseline to 12 weeks (tolterodine, P < 0.0001, and intravaginal estradiol, P = 0.002). Secondary outcome improvement within groups was noted in the HRQL total, urinary incontinence episodes, and median voiding frequency (all P ≤ 0.03) in the tolterodine group and in the HRQL total score (P = 0.03) in the intravaginal estradiol group, with no differences between groups. Combined therapy outcomes at 24 and 52 weeks compared with single therapy at 12 weeks revealed significant improvement in symptom bother score in the intravaginal estradiol + tolterodine group at 24 and 52 weeks (20.0 ± 23.9, P = 0.008; -16.7 ± 23.3, P = 0.02, respectively).
Significant within-group improvement in OAB-q symptom bother was noted in both the intravaginal estradiol and tolterodine groups for OAB symptoms, with no difference between groups. Greater improvement from 12-week single therapy to 24 and 52 weeks of combined therapy was noted in the group originally assigned to intravaginal estradiol. The role of combined medical therapy for OAB symptoms needs further investigation.
本研究旨在比较单药治疗托特罗定(得妥长效)缓释剂与阴道内雌激素(雌二醇)治疗膀胱过度活动症(OAB)症状的12周疗效,并描述接受联合治疗女性的24周和52周疗效。
对有尿频、尿急、夜尿症和/或急迫性尿失禁症状的女性进行单中心随机、开放标签试验。58名参与者被随机分为每日口服托特罗定缓释剂或每晚阴道内使用雌二醇乳膏,持续6周,然后每周两次。主要结局是12周时膀胱过度活动症问卷(OAB-q)症状困扰评分的变化。次要结局包括OAB-q的健康相关生活质量问卷(HRQL)和3天膀胱日记。在12周时,为受试者提供另一种治疗方法,并在24周和52周进行随访。
从基线到12周,托特罗定组和阴道内雌二醇组在症状困扰评分改善方面无差异(分别为20.6±21.7、-15.8±23.3,P = 0.45)。从基线到12周,两组内症状困扰评分均显著下降(托特罗定组,P < 0.0001;阴道内雌二醇组,P = 0.002)。托特罗定组在HRQL总分、尿失禁发作次数和平均排尿频率方面(均P≤0.03)以及阴道内雌二醇组在HRQL总分方面(P = 0.03)的组内次要结局有改善,两组之间无差异。与12周单药治疗相比,24周和52周联合治疗的结果显示,阴道内雌二醇+托特罗定组在24周和52周时症状困扰评分有显著改善(分别为20.0±23.9,P = 0.008;-16.7±日3.3,P = 0.02)。
阴道内雌二醇组和托特罗定组在OAB症状的OAB-q症状困扰方面均有显著的组内改善,两组之间无差异。最初分配接受阴道内雌二醇治疗的组从12周单药治疗到24周和52周联合治疗有更大改善。联合药物治疗对OAB症状的作用需要进一步研究。