Enatsu Rei, Mikuni Nobuhiro
Department of Neurosurgery, Sapporo Medical University.
Neurol Med Chir (Tokyo). 2016 May 15;56(5):221-7. doi: 10.2176/nmc.ra.2015-0319. Epub 2016 Mar 4.
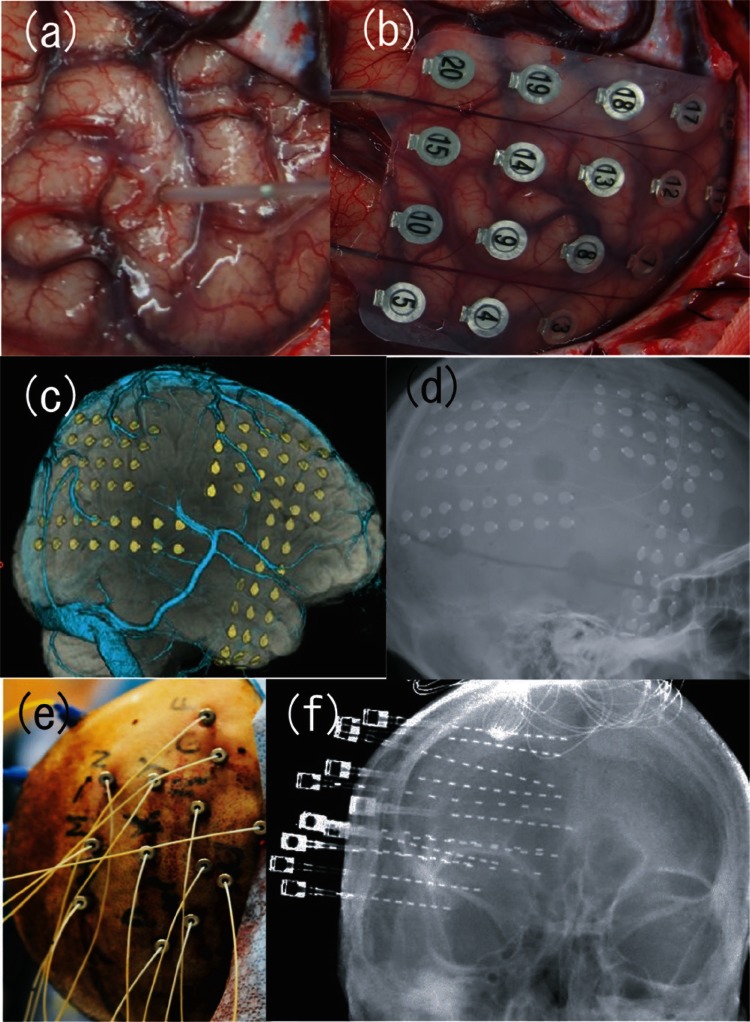
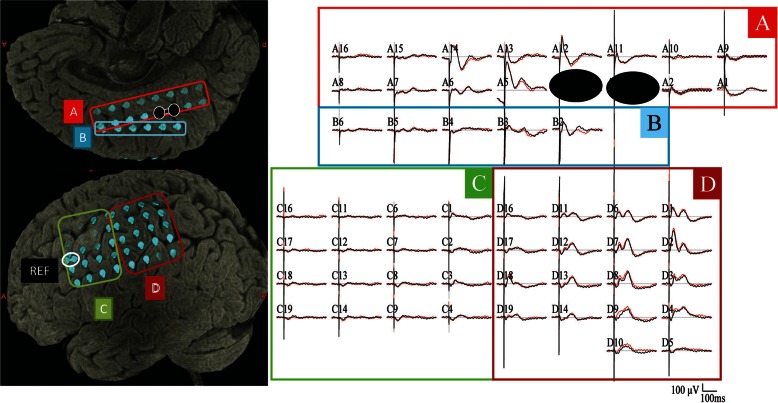
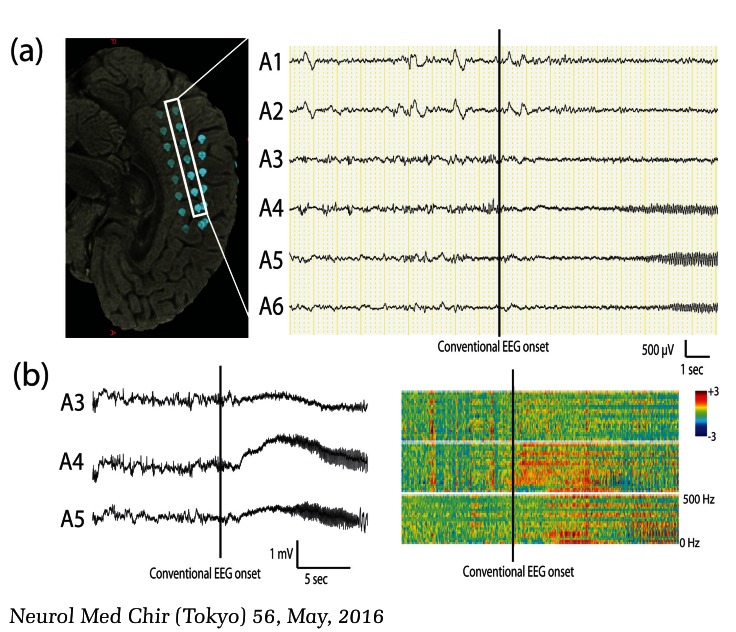
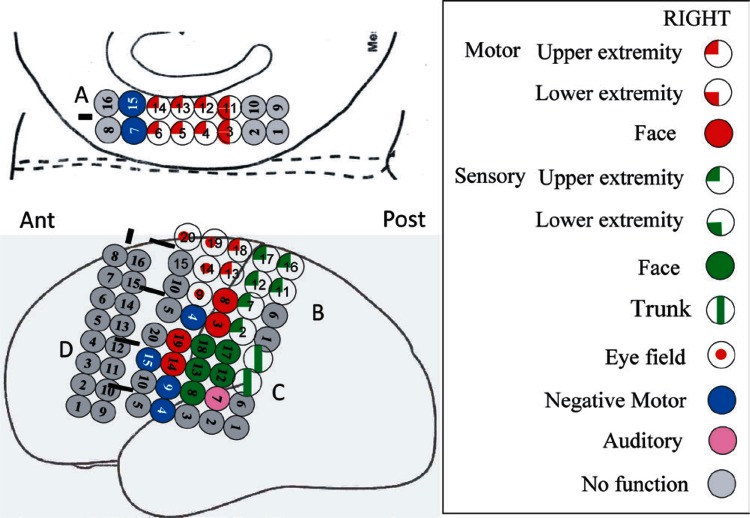
Invasive evaluations play important roles in identifying epileptogenic zones and functional areas in patients with intractable focal epilepsy. This article reviews the usefulness, methods, and limitations of invasive evaluations for epilepsy surgery. Invasive evaluations include various types of intracranial electrodes such as stereotactically implanted intracranial depth electrodes (stereo-EEG), chronic subdural electrodes, and intraoperative electrocorticography. Scalp EEG is distorted by the skull, meninges, and skin. On the other hand, intracranial electrodes provide spatial information with higher resolution than scalp electrodes, thereby enabling further delineation of epileptogenic zones and mapping of functional areas with electrical stimulation. In addition, intracranial electrodes record a wide frequency range of electrical activity, which is not possible with scalp electrodes. The very slow potentials in ictal recordings, known as ictal direct current (DC) shifts and ictal/interictal high frequency oscillations, such as ripples (100-200 Hz) and fast ripples (200-500 Hz), have been correlated with the ictal onset zone and are a sensitive and specific marker for epileptogenicity. Furthermore, several studies reported that the electrical stimulation of epileptogenic zones elicited enhanced cortical evoked potentials, abnormal delayed or repetitive responses, and fast ripples. These responses may assist in the delineation of the epileptogenic cortex as a potential new marker. There are definite risks of complications associated with the use of intracranial electrodes. However, when an invasive evaluation is selected based on careful consideration of the risks and benefits, it provides useful information for establishing a strategy for epilepsy surgery.
侵入性评估在确定难治性局灶性癫痫患者的致痫区和功能区方面发挥着重要作用。本文综述了癫痫手术侵入性评估的实用性、方法及局限性。侵入性评估包括各种类型的颅内电极,如立体定向植入的颅内深部电极(立体脑电图)、慢性硬膜下电极和术中皮质脑电图。头皮脑电图会受到颅骨、脑膜和皮肤的干扰。另一方面,颅内电极提供的空间信息分辨率高于头皮电极,从而能够进一步描绘致痫区并通过电刺激绘制功能区图谱。此外,颅内电极可记录较宽频率范围的电活动,这是头皮电极无法做到的。发作期记录中非常缓慢的电位,即发作期直流(DC)偏移以及发作期/发作间期高频振荡,如涟漪(100 - 200Hz)和快速涟漪(200 - 500Hz),已被证实与发作起始区相关,是致痫性的敏感且特异标志物。此外,多项研究报道,对致痫区进行电刺激会引发增强的皮质诱发电位、异常延迟或重复反应以及快速涟漪。这些反应可能有助于将致痫皮质描绘为一种潜在的新标志物。使用颅内电极存在一定的并发症风险。然而,当基于对风险和益处的仔细权衡选择侵入性评估时,它可为制定癫痫手术策略提供有用信息。