Ramaswami Uma, Cooper Jackie, Humphries Steve E
Lysosomal Disorders Unit, Royal Free Hospital, London, UK.
British Heart Foundation Laboratories, Centre for Cardiovascular Genetics, Institute of Cardiovascular Science, the Rayne Building University College London, London, UK.
Arch Dis Child. 2017 Mar;102(3):255-260. doi: 10.1136/archdischild-2015-308570. Epub 2016 Mar 6.
The National Institute for Health and Care Excellence 2008 guidelines on the treatment and management of familial hypercholesterolaemia (FH) recommend that children with FH should be considered for statin treatment by the age of 10 years. The Paediatric FH Register was established in 2012 to collect baseline and long-term follow-up data on all children with FH in the UK.
Paediatricians and adult lipidologists have been invited to enter baseline data on any child with a clinical diagnosis of FH using an electronic capture record.
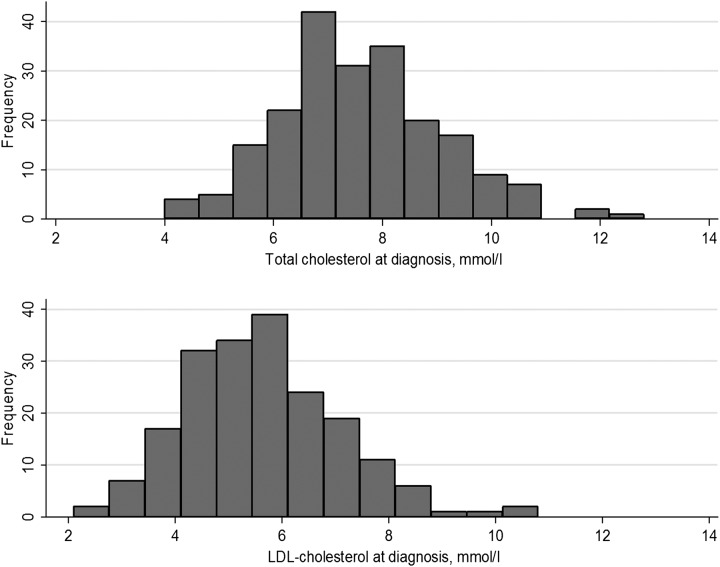
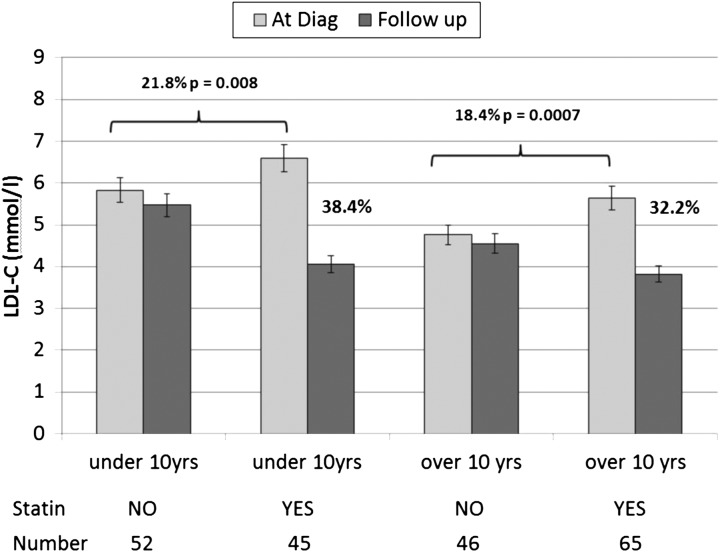
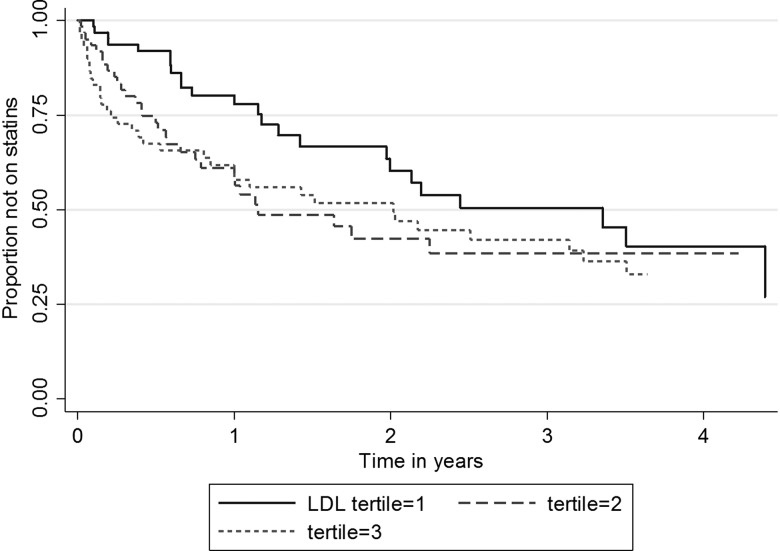
Baseline data is on 232 children (50% boys, 80% Caucasian), with an untreated mean (SD) total cholesterol of 7.61 (1.48) mmol/L and low-density lipoprotein cholesterol (LDL-C) of 5.67 (1.46) mmol/L. Overall 111/232 (47.8%) of the children were on statins. Children over the age of 10 years at the most recent follow-up were twice as likely to be on statin treatment than those under 10 years (57.6% (102/177) vs 23.1% (9/39), p=0.00009). In both age groups, those subsequently on statin treatment had significantly higher diagnostic total and LDL-C (overall 6.01 (1.46) mmol/L vs 5.31 (1.37) mmol/L, p=0.00007), and had stronger evidence of a family history of early coronary heart disease (CHD) in parent or first-degree relative (overall 28.4% vs 19.0%, p=0.09). In statin-treated children LDL-C level was reduced by 35% (2.07 (1.38) mmol/L) compared with a reduction of 5.5% (0.29 (0.87) mmol/L), p=0.0001 in those not treated. None of those on statin had measured plasma levels of creatine kinase, alanine aminotransferase and AST indicative of statin toxicity (ie, >2.5 times the upper limit of the normal range).
The data indicates that treatment decisions in children with FH are appropriately based on a stronger family history of CHD and higher LDL-C.
英国国家卫生与临床优化研究所(National Institute for Health and Care Excellence)2008年发布的关于家族性高胆固醇血症(FH)治疗与管理的指南建议,FH患儿应在10岁时考虑使用他汀类药物治疗。儿童FH登记册于2012年建立,用于收集英国所有FH患儿的基线数据和长期随访数据。
已邀请儿科医生和成人脂质专家使用电子采集记录录入任何临床诊断为FH的儿童的基线数据。
共收集了232名儿童的基线数据(50%为男孩,80%为白种人),未治疗时平均(标准差)总胆固醇为7.61(1.48)mmol/L,低密度脂蛋白胆固醇(LDL-C)为5.67(1.46)mmol/L。总体而言,232名儿童中有111名(47.8%)正在服用他汀类药物。在最近一次随访中,年龄超过10岁的儿童接受他汀类药物治疗的可能性是10岁以下儿童的两倍(57.6%(102/177)对23.1%(9/39),p=0.00009)。在两个年龄组中,随后接受他汀类药物治疗的儿童诊断时的总胆固醇和LDL-C显著更高(总体分别为6.01(1.46)mmol/L对5.31(1.37)mmol/L,p=0.00007),并且有更强的证据表明父母或一级亲属有早发性冠心病(CHD)家族史(总体分别为28.4%对19.0%,p=0.09)。在接受他汀类药物治疗的儿童中,LDL-C水平降低了35%(降至2.07(1.38)mmol/L),而未接受治疗的儿童降低了5.5%(降至0.29(0.87)mmol/L),p=0.0001。接受他汀类药物治疗的儿童中,没有测量到提示他汀类药物毒性的肌酸激酶、丙氨酸转氨酶和天冬氨酸转氨酶的血浆水平(即高于正常范围上限的2.5倍)。
数据表明,FH患儿的治疗决策适当地基于更强的CHD家族史和更高的LDL-C水平。