Fukui Tomoya, Itabashi Michiko, Ishihara Mikiko, Hiyoshi Yasuhiro, Kasajima Masashi, Igawa Satoshi, Sasaki Jiichiro, Masuda Noriyuki
Department of Respiratory Medicine, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa, 252-0374, Japan.
Research and Development Center for New Medical Frontiers, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa, 252-0374, Japan.
BMC Cancer. 2016 Mar 8;16:197. doi: 10.1186/s12885-016-2222-4.
The efficacy of combined modality therapy is evaluated for patients with extensive-stage (ES) small cell lung cancer (SCLC). This study evaluated prognostic factors affecting the risk of thoracic progression in ES-SCLC patients likely to undergo thoracic radiotherapy combined chemotherapy.
A retrospective review of ES-SCLC patients who had received systemic chemotherapy at our hospital was performed. Tumor size, metastatic sites, and laboratory data at diagnosis were evaluated as potential prognostic factors. In ES-SCLC patients without pleural dissemination, the rate of thoracic progression after initial chemotherapy was assessed.
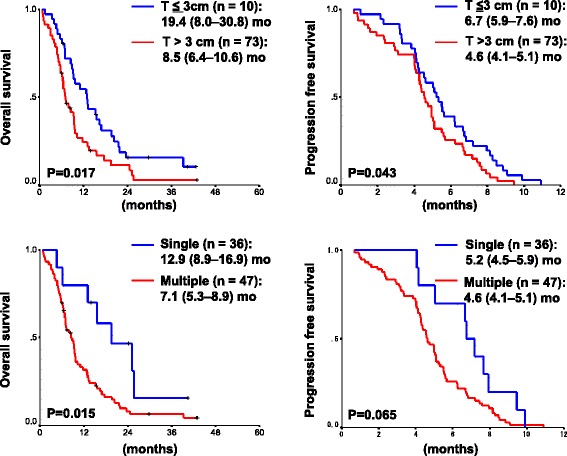
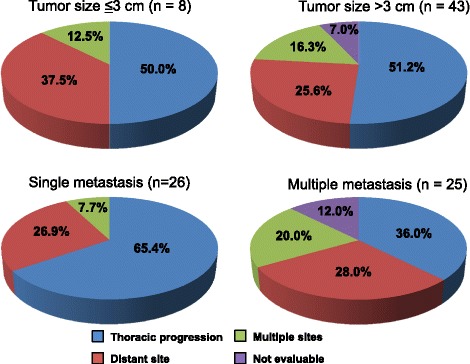
Eighty-three of 96 consecutive ES-SCLC patients were analyzed. The overall response rate was 55 %, median progression free survival was 5.0 months (mo), and overall survival (OS) was 9.2 mo. Tumor size (19.4 mo for ≤3 cm vs. 8.5 mo for >3 cm, p = 0.017) and the number of metastatic sites (12.9 mo for single sites vs. 7.1 mo for multiple sites, p = 0.015) were prognostic factors, in addition to known prognostic factors such as performance status and the levels of LDH and sodium. Cox proportional hazard model showed that the OS was significantly worse in patients with large (>3 cm) primary tumor size {HR 2.44 [95 % confidential interval (CI) 1.05-5.68], p = 0.038} and multiple metastatic sites [HR 1.81 (95 % CI 1.08-3.04), p = 0.026]. In 51 cases without pleural dissemination, the number of metastatic sites was associated with thoracic progression after initial chemotherapy (65 % for single sites vs. 36 % for multiple sites, p = 0.036).
Large tumor size and multiple metastatic sites at diagnosis significantly predicted poor survival in ES-SCLC patients. Based on the high rate of thoracic progression in ES-SCLC patients with single site of distant metastasis, we should consider thoracic radiotherapy combined with chemotherapy for this population.
对广泛期(ES)小细胞肺癌(SCLC)患者联合治疗的疗效进行评估。本研究评估了影响可能接受胸部放疗联合化疗的ES-SCLC患者胸部进展风险的预后因素。
对我院接受全身化疗的ES-SCLC患者进行回顾性分析。将诊断时的肿瘤大小、转移部位和实验室数据作为潜在的预后因素进行评估。对无胸膜播散的ES-SCLC患者,评估初始化疗后的胸部进展率。
对连续96例ES-SCLC患者中的83例进行分析。总缓解率为55%,中位无进展生存期为5.0个月(mo),总生存期(OS)为9.2 mo。除了已知的预后因素如体能状态、乳酸脱氢酶和钠水平外,肿瘤大小(≤3 cm者为19.4 mo,>3 cm者为8.5 mo,p = 0.017)和转移部位数量(单部位者为12.9 mo,多部位者为7.1 mo,p = 0.015)也是预后因素。Cox比例风险模型显示,原发肿瘤大(>3 cm)的患者OS显著更差{风险比(HR)2.44 [95%置信区间(CI)1.05 - 5.68],p = 0.038},转移部位多的患者也是如此[HR 1.81(95% CI 1.08 - 3.04),p = 0.026]。在51例无胸膜播散的患者中,转移部位数量与初始化疗后的胸部进展相关(单部位者为65%,多部位者为36%,p = 0.036)。
诊断时肿瘤大及转移部位多显著预示ES-SCLC患者生存不良。基于远处转移单部位的ES-SCLC患者胸部进展率高,我们应考虑对该人群采用胸部放疗联合化疗。