McCarthy Helen S, Richardson James B, Parker Jane C E, Roberts Sally
Centre for Spinal Studies, Robert Jones and Agnes Orthopaedic Hospital NHS Foundation Trust, Oswestry, Shropshire, UK; ISTM, Keele University, Keele, Staffordshire, UK.
ISTM, Keele University, Keele, Staffordshire, UK; Institute of Orthopaedics, Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust, Oswestry, Shropshire, UK.
Cartilage. 2016 Jan;7(1):7-15. doi: 10.1177/1947603515607963.
To establish if harvesting cartilage to source chondrocytes for autologous chondrocyte implantation (ACI) results in donor site morbidity.
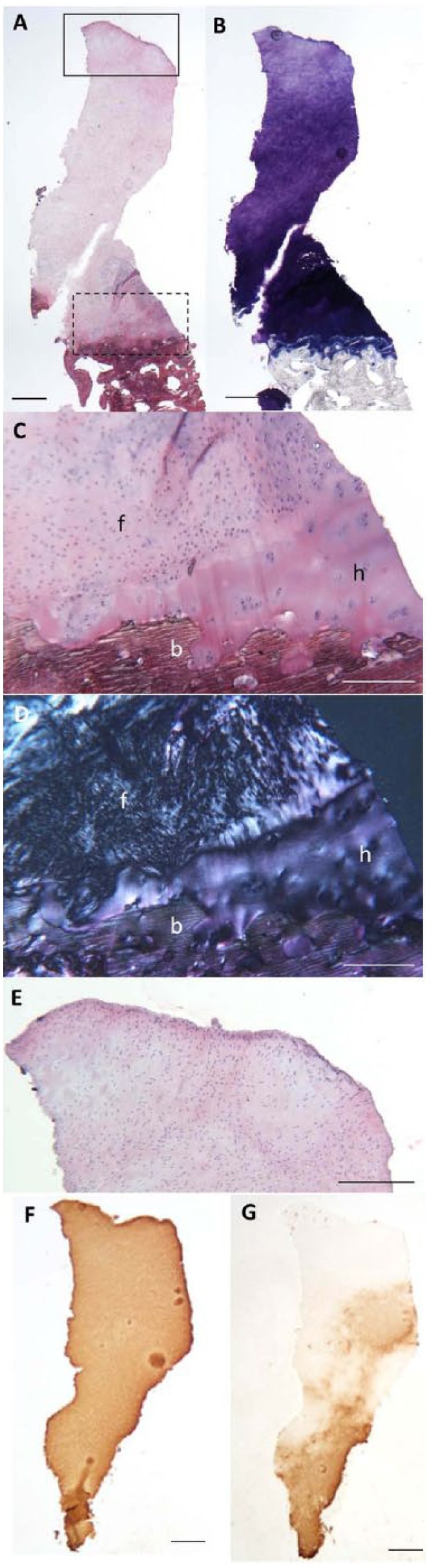
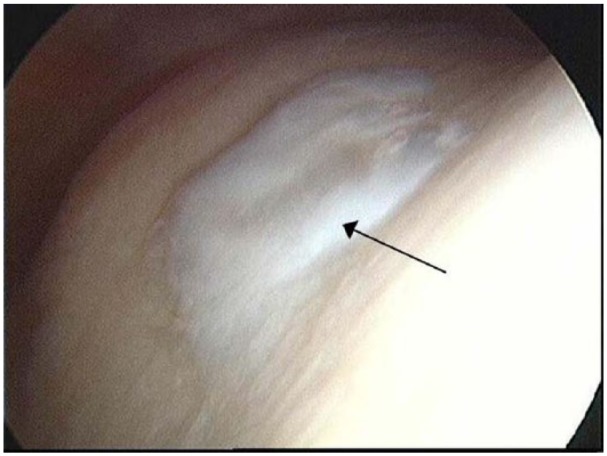
Twenty-three patients underwent ACI for chondral defects of either the ankle or the hip. This involved cartilage harvest from the knee (stage I), chondrocyte expansion in the laboratory and implantation surgery (stage II) into the affected joint. Prior to chondral harvest, no patient had sought treatment for their knee. Lysholm knee scores were completed prior to chondral harvest and annually post-ACI. Histological analyses of the donor site were performed at 12.3 ± 1.5 months for 3 additional patients who had previously had ACI of the knee.
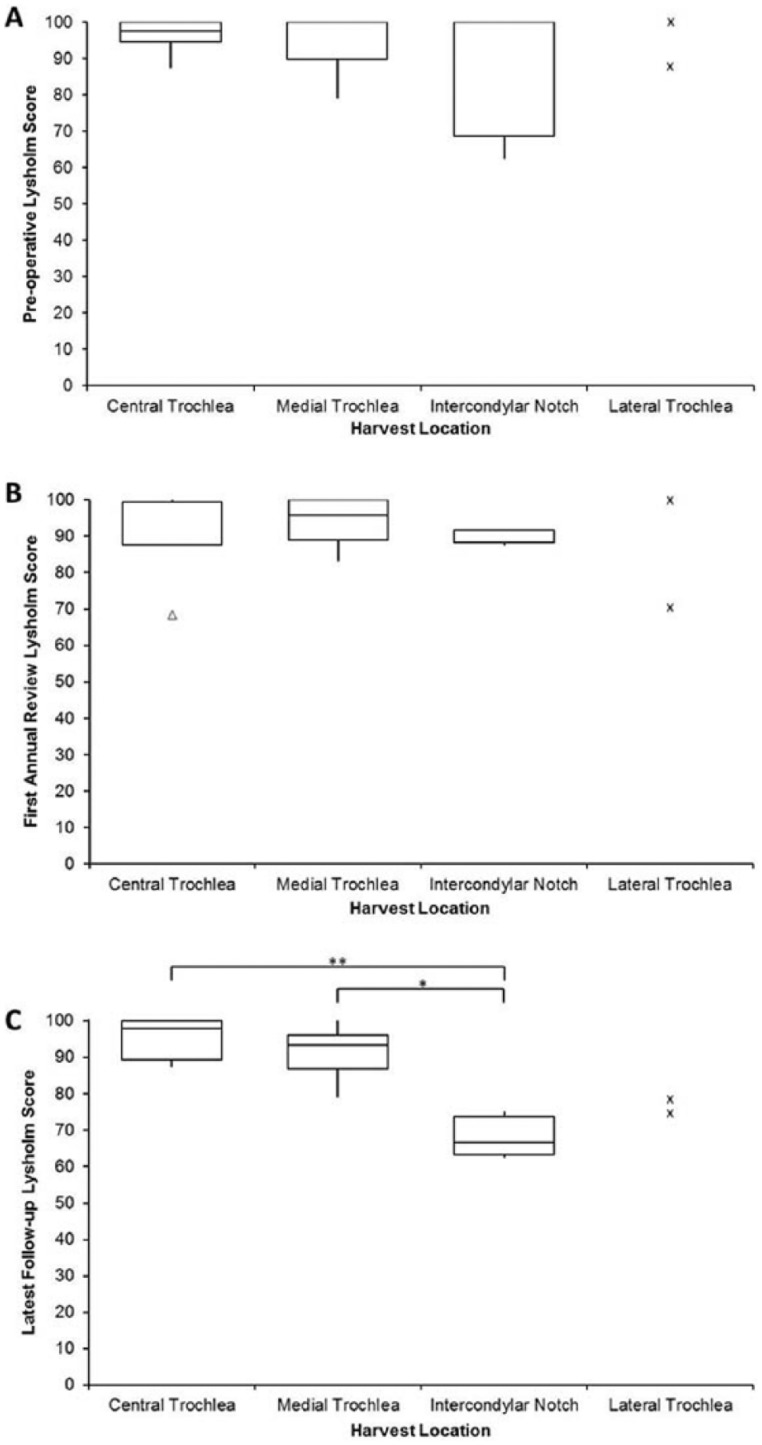
The median preoperative Lysholm score was 100, with no significant differences observed at either 13.7±1.7 months or 4.8±1.8 years postharvest (median Lysholm scores 91.7 and 87.5, respectively). Patients whose cartilage was harvested from the central or medial trochlea had a significantly higher median Lysholm score at latest follow-up (97.9 and 93.4, respectively), compared with those taken from the intercondylar notch (median Lysholm score 66.7). The mean International Cartilage Repair Society (ICRS) II histological score for the biopsies taken from the donor site of 3 additional knee ACI patients was 117 ± 10 (maximum score 140).
This study suggests that the chondral harvest site in ACI is not associated with significant joint morbidity, at least up to 5 years postharvest. However, one should carefully consider the location for chondral harvest as this has been shown to affect knee function in the longer term.
确定采集软骨以获取软骨细胞用于自体软骨细胞移植(ACI)是否会导致供区并发症。
23例患者因踝关节或髋关节软骨损伤接受ACI治疗。这包括从膝关节采集软骨(I期),在实验室中扩增软骨细胞并进行植入手术(II期)至受影响关节。在采集软骨前,没有患者因膝关节问题寻求治疗。在采集软骨前及ACI术后每年完成Lysholm膝关节评分。对另外3例先前接受过膝关节ACI治疗的患者,在12.3±1.5个月时对供区进行组织学分析。
术前Lysholm评分中位数为100,采集后13.7±1.7个月或4.8±1.8年时均未观察到显著差异(Lysholm评分中位数分别为91.7和87.5)。与从髁间切迹采集软骨的患者相比,从中央或内侧滑车采集软骨的患者在最近一次随访时Lysholm评分中位数显著更高(分别为97.9和93.4),而从髁间切迹采集软骨的患者Lysholm评分中位数为66.7。另外3例膝关节ACI患者供区活检的国际软骨修复协会(ICRS)II级组织学评分均值为117±10(满分140)。
本研究表明,ACI中的软骨采集部位与显著的关节并发症无关,至少在采集后5年内如此。然而,应仔细考虑软骨采集的位置,因为已表明这会在长期影响膝关节功能。