Pokrovska Tzveta, Jones Jeremy, Shaikh M Guftar, Smith Sarah, Donaldson Malcolm D C
Section of Child Health, University of Glasgow School of Medicine, Royal Hospital for Children, Queen Elizabeth University Hospital, Glasgow, UK.
NHS Greater Glasgow and Clyde, Royal Hospital for Children, Queen Elizabeth University Hospital, Glasgow, UK.
Arch Dis Child. 2016 Jun;101(6):539-545. doi: 10.1136/archdischild-2015-309529. Epub 2016 Mar 10.
To determine, in newborn infants referred with elevated capillary thyroid-stimulating hormone (TSH), a threshold below which a frankly subnormal venous free thyroxine (fT4) level of <10 pmol/L is unlikely, so that treatment with levo-thyroxine (L-T4) might be deferred until venous thyroid function tests (TFTs) become available.
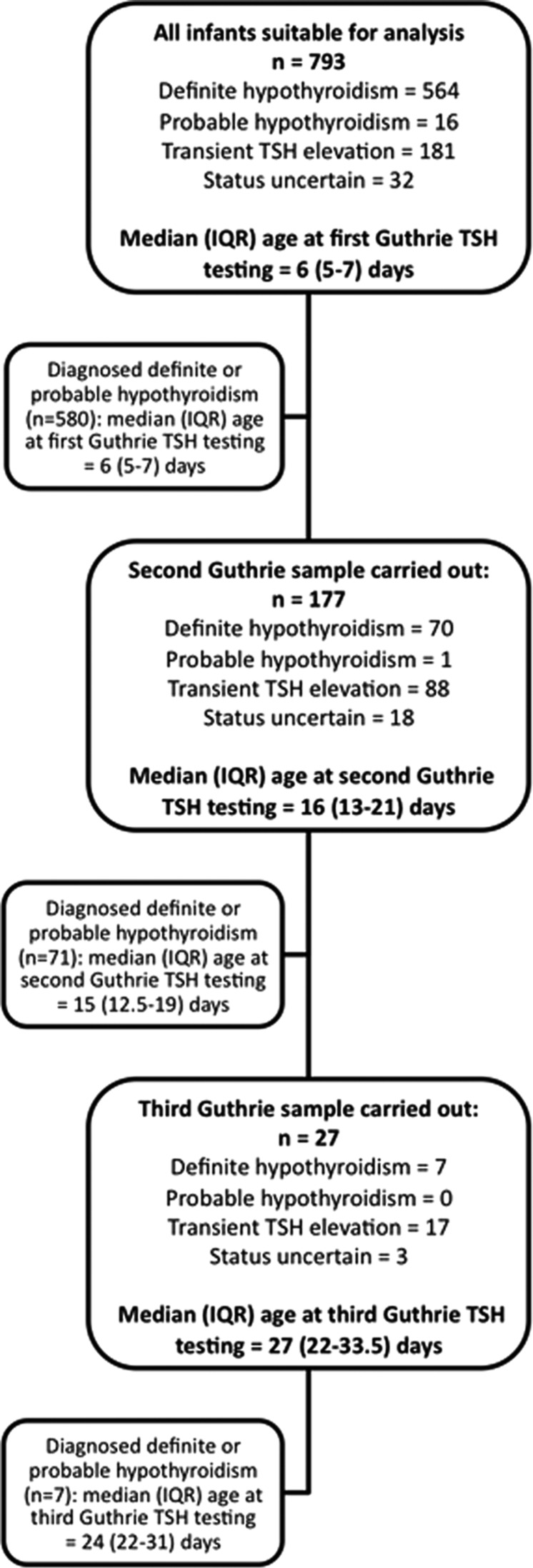
All infants referred in Scotland since 1979 with capillary TSH elevation were studied, with particular focus on infants screened using the AutoDELFIA assay between 2002 and 2013.
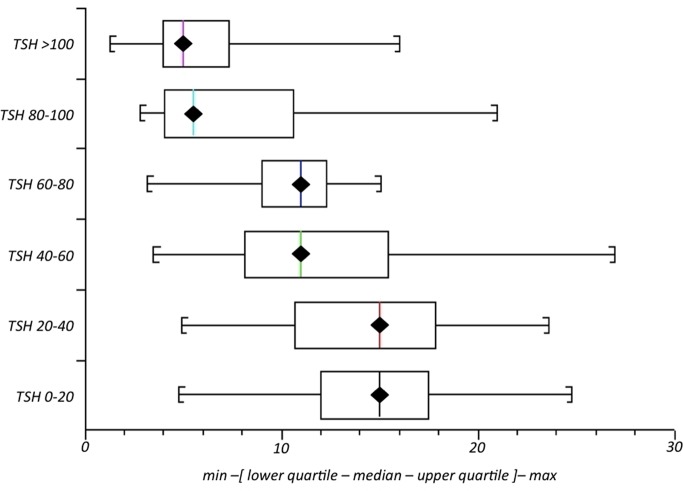
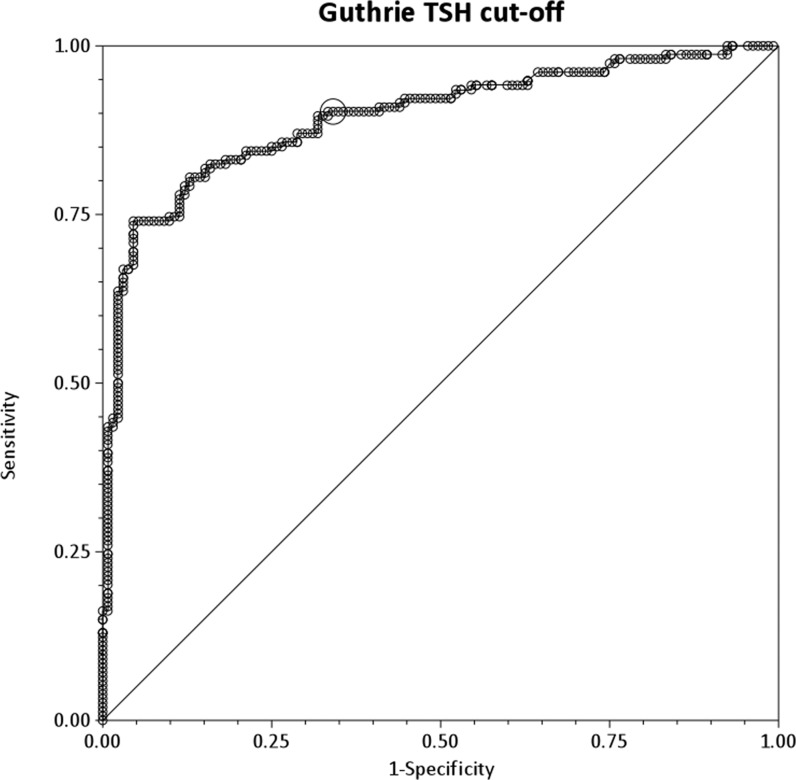
Of the 321 infants referred with capillary TSH elevation using AutoDELFIA, 35 were excluded (fT4/TSH unavailable (12), venous sample either preceding or >10 days after capillary sampling (13, 10)), leaving 286 eligible for analysis (208 definite/probable hypothyroidism, 61 transient TSH elevation, 17 of uncertain thyroid status). Capillary TSH and venous T4 were strongly correlated (Spearman's rank correlation coefficient -0.707355). The optimal capillary TSH threshold for predicting a venous fT4 of <10 pmol/L was found to be >40 mU/L (90.3% sensitivity and 65.9% specificity compared with 90.25% and 59.1% for >35 mU/L and 88.3% and 68.2% for >45 mU/L). 93 infants (32.5%) had capillary TSH ≤40 mU/L at referral of whom 15 (9.7%) had venous fT4 <10 pmol/L, comprising seven with true congenital hypothyroidism, five with transient TSH elevation and three with uncertain status, two of whom died.
For infants in whom capillary TSH is ≤40 mU/L, it is reasonable to defer L-T4 treatment until venous TFT results are known provided that the latter become available quickly.
在因毛细血管促甲状腺激素(TSH)升高而转诊的新生儿中,确定一个阈值,低于该阈值时不太可能出现明显低于正常水平的静脉游离甲状腺素(fT4)<10 pmol/L,以便在静脉甲状腺功能检查(TFT)结果出来之前可推迟左甲状腺素(L-T4)治疗。
研究了自1979年以来在苏格兰因毛细血管TSH升高而转诊的所有婴儿,特别关注2002年至2013年期间使用AutoDELFIA检测法筛查的婴儿。
在321例因毛细血管TSH升高而使用AutoDELFIA转诊的婴儿中,35例被排除(无法获得fT4/TSH数据(12例),静脉样本在毛细血管采样之前或之后超过10天(13例、10例)),剩下286例符合分析条件(208例确诊/可能的甲状腺功能减退症,61例短暂性TSH升高,17例甲状腺状态不确定)。毛细血管TSH与静脉T4密切相关(斯皮尔曼等级相关系数-0.707355)。预测静脉fT4<10 pmol/L的最佳毛细血管TSH阈值为>40 mU/L(敏感性为90.3%,特异性为65.9%,相比之下,>35 mU/L时分别为90.25%和59.1%,>45 mU/L时分别为88.3%和68.2%)。93例婴儿(32.5%)在转诊时毛细血管TSH≤40 mU/L,其中15例(9.7%)静脉fT_{4}<10 pmol/L,包括7例真正的先天性甲状腺功能减退症、5例短暂性TSH升高和3例状态不确定者,其中2例死亡。
对于毛细血管TSH≤40 mU/L的婴儿,如果能很快获得静脉TFT结果,推迟L-T4治疗直到结果出来是合理的。