Su Alvin W, Habermann Elizabeth B, Thomsen Kristine M, Milbrandt Todd A, Nassr Ahmad, Larson A Noelle
Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN.
National Yang-Ming University, Taipei, Taiwan.
Spine (Phila Pa 1976). 2016 Oct 1;41(19):1523-1534. doi: 10.1097/BRS.0000000000001558.
Retrospective review of a prospective cohort.
The aim of the study was to determine the patient characteristics and surgical procedure factors related to increased rates of 30-day unplanned readmission and major perioperative complications after spinal fusion surgery, and the association between unplanned readmission and major complications.
Reducing unplanned readmissions can reduce the cost of healthcare. Payers are implementing penalties for 30-day readmissions after discharge. There is limited data regarding the current rates and risk factors for unplanned readmission and major complications related to spinal fusion surgery.
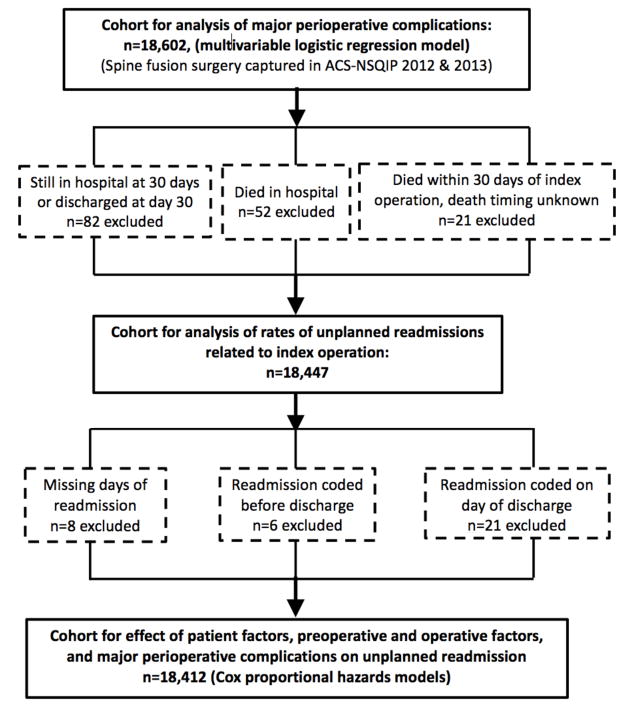
Spine fusion patients were identified using the 2012 and 2013 American College of Surgeons National Surgical Quality Improvement Program Participant User File. Rates of readmissions within 30 days after spine fusion surgery were calculated using the person-years method. Cox proportional hazards models were used to assess the independent associations of spine surgical procedure types, diagnoses, patient profiles, and major perioperative complications with unplanned related readmissions. Independent risk factors for major complications were assessed by multivariable logistic regression.
Of the 18,602 identified patients, there was a 5.2% overall major perioperative complication rate. There was a rate of 4.4% per 30 person-days for unplanned readmissions related to index surgery. Independent risk factors for both readmissions and major perioperative complications included combined anterior and posterior surgery, diagnosis of solitary tumor, older age, and higher American Society of Anesthesiologists class. Patients with deep/organ surgical site infection carried higher risk of having unplanned readmission, followed by pulmonary embolism, acute renal failure, and stroke/cerebral vascular accident with neurological deficit.
This study provides benchmark rates of 30-day readmission based on diagnosis and procedure codes from a high-quality database for adult spinal fusion patients and showed increased rates of 30-day unplanned readmission and major perioperative complications for patients with specific risk factors. Targeted preoperative planning on modifiable risk factors with proportional reimbursement may promote higher-quality healthcare.
对前瞻性队列进行回顾性分析。
本研究旨在确定与脊柱融合手术后30天内非计划再入院率和主要围手术期并发症发生率增加相关的患者特征和手术因素,以及非计划再入院与主要并发症之间的关联。
降低非计划再入院率可降低医疗成本。支付方正在对出院后30天内的再入院实施处罚。关于脊柱融合手术当前的非计划再入院率及相关危险因素和主要并发症的数据有限。
使用2012年和2013年美国外科医师学会国家外科质量改进计划参与者用户文件识别脊柱融合患者。采用人年法计算脊柱融合手术后30天内的再入院率。使用Cox比例风险模型评估脊柱手术类型、诊断、患者概况和主要围手术期并发症与非计划相关再入院的独立关联。通过多变量逻辑回归评估主要并发症的独立危险因素。
在18,602例已识别患者中,总体主要围手术期并发症发生率为5.2%。与初次手术相关的非计划再入院率为每30人日4.4%。再入院和主要围手术期并发症的独立危险因素包括前后联合手术、孤立性肿瘤诊断、年龄较大以及美国麻醉医师协会分级较高。深部/器官手术部位感染患者发生非计划再入院的风险较高,其次是肺栓塞、急性肾衰竭以及伴有神经功能缺损的中风/脑血管意外。
本研究基于高质量数据库中成人脊柱融合患者的诊断和手术编码提供了30天再入院的基准率,并显示具有特定危险因素的患者30天非计划再入院率和主要围手术期并发症发生率增加。针对可改变的危险因素进行有针对性的术前规划并给予相应报销,可能会促进更高质量的医疗保健。
3级。