Taylor Natalie, Long Janet C, Debono Deborah, Williams Rachel, Salisbury Elizabeth, O'Neill Sharron, Eykman Elizabeth, Braithwaite Jeffrey, Chin Melvin
Centre for Healthcare Resilience and Implementation Science, Australian Institute of Health Innovation, Faculty of Medicine and Health, Macquarie University, Sydney, NSW, 2109, Australia.
Prince of Wales Hospital, Sydney, NSW, Australia.
BMC Health Serv Res. 2016 Mar 12;16:89. doi: 10.1186/s12913-016-1331-8.
Lynch syndrome is an inherited disorder associated with a range of cancers, and found in 2-5 % of colorectal cancers. Lynch syndrome is diagnosed through a combination of significant family and clinical history and pathology. The definitive diagnostic germline test requires formal patient consent after genetic counselling. If diagnosed early, carriers of Lynch syndrome can undergo increased surveillance for cancers, which in turn can prevent late stage cancers, optimise treatment and decrease mortality for themselves and their relatives. However, over the past decade, international studies have reported that only a small proportion of individuals with suspected Lynch syndrome were referred for genetic consultation and possible genetic testing. The aim of this project is to use behaviour change theory and implementation science approaches to increase the number and speed of healthcare professional referrals of colorectal cancer patients with a high-likelihood risk of Lynch syndrome to appropriate genetic counselling services.
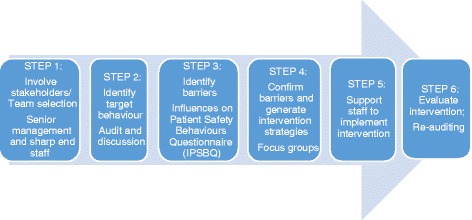
The six-step Theoretical Domains Framework Implementation (TDFI) approach will be used at two large, metropolitan hospitals treating colorectal cancer patients. Steps are: 1) form local multidisciplinary teams to map current referral processes; 2) identify target behaviours that may lead to increased referrals using discussion supported by a retrospective audit; 3) identify barriers to those behaviours using the validated Influences on Patient Safety Behaviours Questionnaire and TDFI guided focus groups; 4) co-design interventions to address barriers using focus groups; 5) co-implement interventions; and 6) evaluate intervention impact. Chi square analysis will be used to test the difference in the proportion of high-likelihood risk Lynch syndrome patients being referred for genetic testing before and after intervention implementation. A paired t-test will be used to assess the mean time from the pathology test results to referral for high-likelihood Lynch syndrome patients pre-post intervention. Run charts will be used to continuously monitor change in referrals over time, based on scheduled monthly audits.
This project is based on a tested and refined implementation strategy (TDFI approach). Enhancing the process of identifying and referring people at high-likelihood risk of Lynch syndrome for genetic counselling will improve outcomes for patients and their relatives, and potentially save public money.
林奇综合征是一种与多种癌症相关的遗传性疾病,在2%至5%的结直肠癌患者中被发现。林奇综合征通过家族病史、临床病史和病理学综合诊断。明确的诊断性种系检测需要在遗传咨询后获得患者正式同意。如果早期诊断,林奇综合征携带者可加强对癌症的监测,进而预防晚期癌症,优化治疗方案,并降低自身及其亲属的死亡率。然而,在过去十年中,国际研究报告称,只有一小部分疑似林奇综合征的个体被转介进行遗传咨询和可能的基因检测。本项目的目的是运用行为改变理论和实施科学方法,增加医疗专业人员将具有林奇综合征高风险的结直肠癌患者转介至适当遗传咨询服务的数量和速度。
将在两家治疗结直肠癌患者的大型都市医院采用六步理论领域框架实施(TDFI)方法。步骤如下:1)组建当地多学科团队,梳理当前的转介流程;2)通过回顾性审计支持的讨论,确定可能增加转介的目标行为;3)使用经过验证的《对患者安全行为的影响问卷》和TDFI指导的焦点小组,确定这些行为的障碍;4)通过焦点小组共同设计干预措施以消除障碍;5)共同实施干预措施;6)评估干预效果。将使用卡方分析来检验干预实施前后被转介进行基因检测的林奇综合征高风险患者比例的差异。将使用配对t检验来评估干预前后林奇综合征高风险患者从病理检测结果到转介的平均时间。将根据每月定期审计,使用运行图持续监测转介随时间的变化。
本项目基于一种经过测试和完善的实施策略(TDFI方法)。加强对具有林奇综合征高风险的人群进行识别并转介至遗传咨询的过程,将改善患者及其亲属的治疗效果,并有可能节省公共资金。