Mellas John
Department of Internal Medicine, St Mary's Health Center, 6400 Clayton Road, St Louis, Missouri, 63017, United States.
Math Biosci. 2016 May;275:107-14. doi: 10.1016/j.mbs.2016.02.010. Epub 2016 Mar 10.
Acute kidney injury (AKI) is a common and serious condition encountered in hospitalized patients. The severity of kidney injury is defined by the RIFLE, AKIN, and KDIGO criteria which attempt to establish the degree of renal impairment. The KDIGO guidelines state that the creatinine clearance should be measured whenever possible in AKI and that the serum creatinine concentration and creatinine clearance remain the best clinical indicators of renal function. Neither the RIFLE, AKIN, nor KDIGO criteria estimate actual creatinine clearance. Furthermore there are no accepted methods for accurately estimating creatinine clearance (K) in AKI.
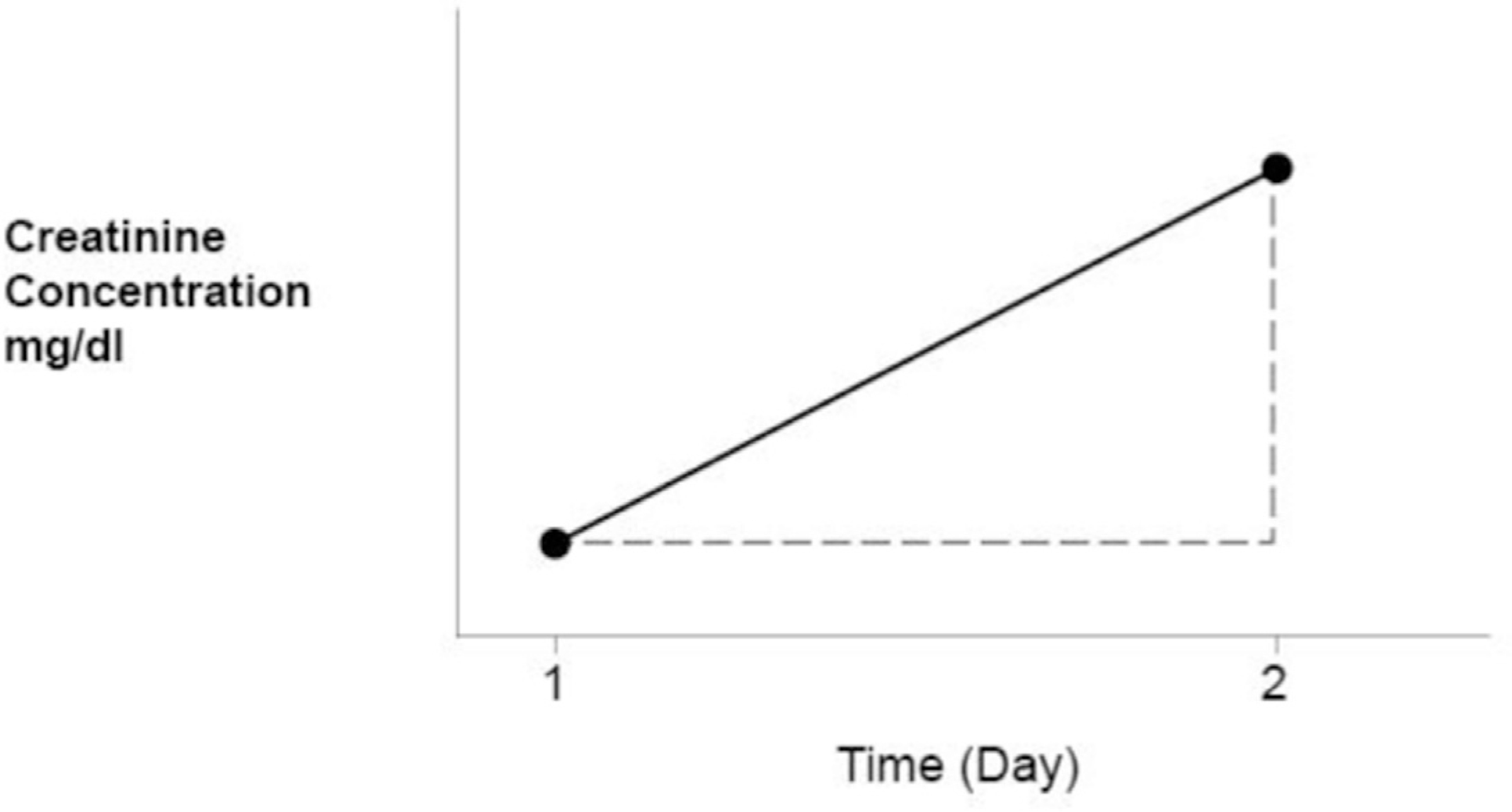
The present study describes a unique method for estimating K in AKI using urine creatinine excretion over an established time interval (E), an estimate of creatinine production over the same time interval (P), and the estimated static glomerular filtration rate (sGFR), at time zero, utilizing the CKD-EPI formula. Using these variables estimated creatinine clearance (Ke)=E/P * sGFR.
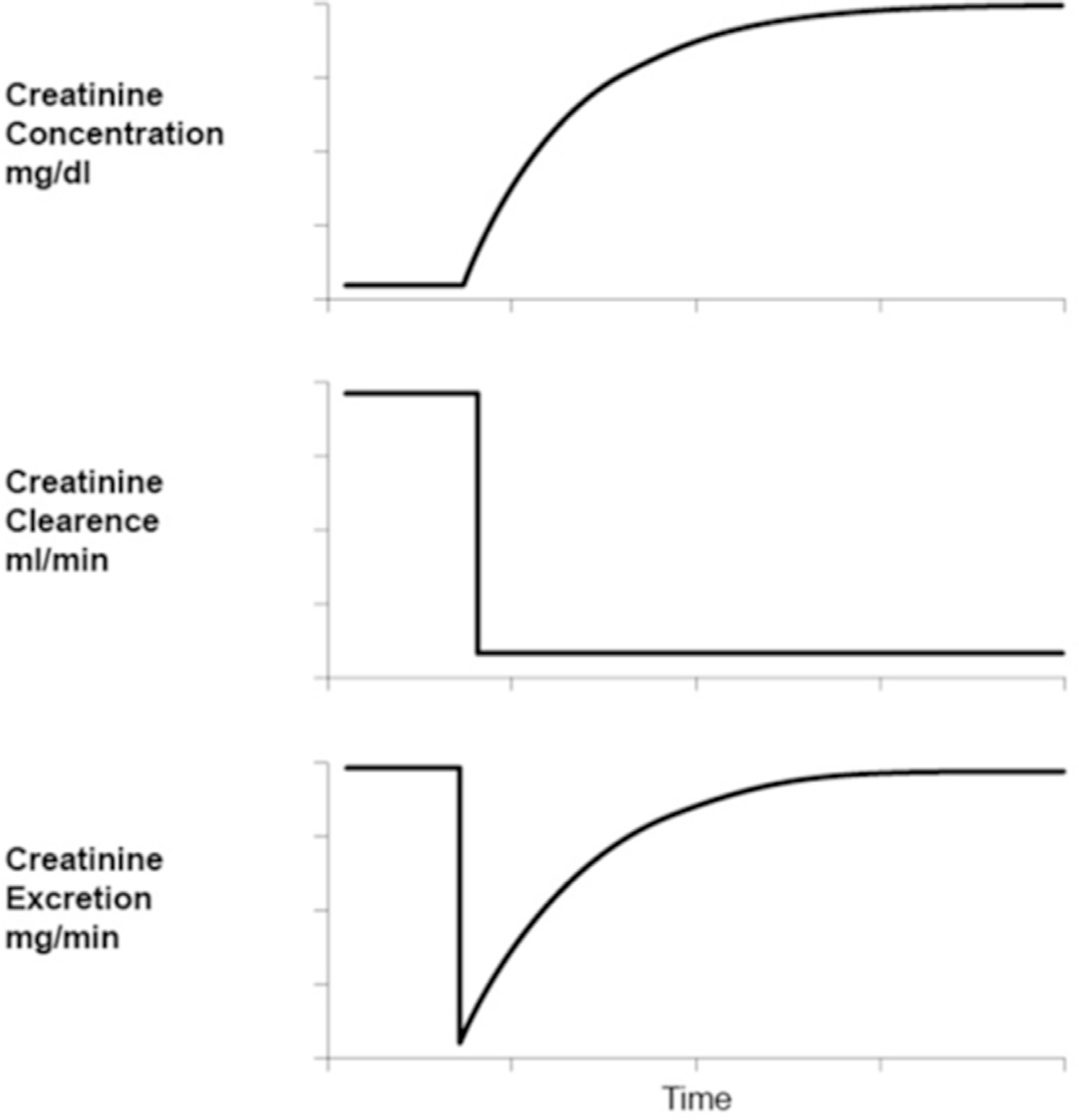
The method was tested for validity using simulated patients where actual creatinine clearance (Ka) was compared to Ke in several patients, both male and female, and of various ages, body weights, and degrees of renal impairment. These measurements were made at several serum creatinine concentrations in an attempt to determine the accuracy of this method in the non-steady state. In addition E/P and Ke was calculated in hospitalized patients, with AKI, and seen in nephrology consultation by the author. In these patients the accuracy of the method was determined by looking at the following metrics; E/P>1, E/P<1, E=P in an attempt to predict progressive azotemia, recovering azotemia, or stabilization in the level of azotemia respectively. In addition it was determined whether Ke<10 ml/min agreed with Ka and whether patients with AKI on renal replacement therapy could safely terminate dialysis if Ke was greater than 5 ml/min.
In the simulated patients there were 96 measurements in six different patients where Ka was compared to Ke. The estimated proportion of Ke within 30% of Ka was 0.907 with 95% exact binomial proportion confidence limits. The predictive accuracy of E/P in the study patients was also reported as a proportion and the associated 95% confidence limits: 0.848 (0.800, 0.896) for E/P<1; 0.939 (0.904, 0.974) for E/P>1 and 0.907 (0.841, 0.973) for 0.9<E/P<1.1. Ke<10 ml/min correlated very well with Ka, while Ke>5 ml/min accurately predicted the ability to terminate renal replacement therapy in AKI.
Include the need to measure urine volume accurately. Furthermore the precision of the method requires accurate estimates of sGFR, while a reasonable measure of P is crucial to estimating Ke.
The present study provides the practitioner with a new tool to estimate real time K in AKI with enough precision to predict the severity of the renal injury, including progression, stabilization, or improvement in azotemia. It is the author's belief that this simple method improves on RIFLE, AKIN, and KDIGO for estimating the degree of renal impairment in AKI and allows a more accurate estimate of K in AKI.
急性肾损伤(AKI)是住院患者中常见且严重的病症。肾损伤的严重程度由RIFLE、AKIN和KDIGO标准定义,这些标准试图确定肾功能损害的程度。KDIGO指南指出,在AKI患者中应尽可能测量肌酐清除率,且血清肌酐浓度和肌酐清除率仍是肾功能的最佳临床指标。RIFLE、AKIN和KDIGO标准均未估算实际的肌酐清除率。此外,目前尚无公认的准确估算AKI患者肌酐清除率(K)的方法。
本研究描述了一种独特的估算AKI患者K值的方法,该方法利用既定时间间隔内的尿肌酐排泄量(E)、同一时间间隔内的肌酐生成量估算值(P)以及利用CKD-EPI公式在时间零点估算的静态肾小球滤过率(sGFR)。利用这些变量,估算的肌酐清除率(Ke)=E/P×sGFR。
该方法通过模拟患者进行有效性测试,将数名不同年龄、体重和肾功能损害程度的男性和女性患者的实际肌酐清除率(Ka)与Ke进行比较。在多个血清肌酐浓度水平下进行这些测量,以确定该方法在非稳态情况下的准确性。此外,还对作者会诊的患有AKI的住院患者计算了E/P和Ke。在这些患者中,通过观察以下指标来确定该方法的准确性:E/P>1、E/P<1、E=P,分别试图预测进行性氮质血症、恢复性氮质血症或氮质血症水平的稳定情况。此外,还确定了Ke<10 ml/min是否与Ka相符,以及AKI患者接受肾脏替代治疗时若Ke大于5 ml/min是否可安全终止透析。
在模拟患者中,对6名不同患者进行了96次测量,比较了Ka与Ke。Ke在Ka的30%范围内的估计比例为0.907,95%精确二项式比例置信区间。研究患者中E/P的预测准确性也以比例形式报告,并给出相关的95%置信区间:E/P<1时为0.848(0.800,0.896);E/P>1时为0.939(0.904,0.974);0.9<E/P<1.1时为0.907(0.841,0.973)。Ke<10 ml/min与Ka相关性非常好,而Ke>5 ml/min准确预测了AKI患者终止肾脏替代治疗的能力。
包括需要准确测量尿量。此外,该方法的精度需要准确估算sGFR,而合理测量P对于估算Ke至关重要。
本研究为临床医生提供了一种新工具,可足够精确地实时估算AKI患者的K值,以预测肾损伤的严重程度,包括氮质血症的进展、稳定或改善情况。作者认为,这种简单方法在估算AKI患者肾功能损害程度方面优于RIFLE、AKIN和KDIGO标准,并能更准确地估算AKI患者的K值。