Bragadottir Gudrun, Redfors Bengt, Ricksten Sven-Erik
Crit Care. 2013 Jun 15;17(3):R108. doi: 10.1186/cc12777.
Estimation of kidney function in critically ill patients with acute kidney injury (AKI), is important for appropriate dosing of drugs and adjustment of therapeutic strategies, but challenging due to fluctuations in kidney function, creatinine metabolism and fluid balance. Data on the agreement between estimating and gold standard methods to assess glomerular filtration rate (GFR) in early AKI are lacking. We evaluated the agreement of urinary creatinine clearance (CrCl) and three commonly used estimating equations, the Cockcroft Gault (CG), the Modification of Diet in Renal Disease (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations, in comparison to GFR measured by the infusion clearance of chromium-ethylenediaminetetraacetic acid (51Cr-EDTA), in critically ill patients with early AKI after complicated cardiac surgery.
Thirty patients with early AKI were studied in the intensive care unit, 2 to 12 days after complicated cardiac surgery. The infusion clearance for 51Cr-EDTA obtained as a measure of GFR (GFR51Cr-EDTA) was calculated from the formula: GFR (mL/min/1.73m2)=(51Cr-EDTA infusion rate×1.73)/(arterial 51Cr-EDTA×body surface area) and compared with the urinary CrCl and the estimated GFR (eGFR) from the three estimating equations. Urine was collected in two 30-minute periods to measure urine flow and urine creatinine. Urinary CrCl was calculated from the formula: CrCl (mL/min/1.73m2)=(urine volume×urine creatinine×1.73)/(serum creatinine×30 min×body surface area).
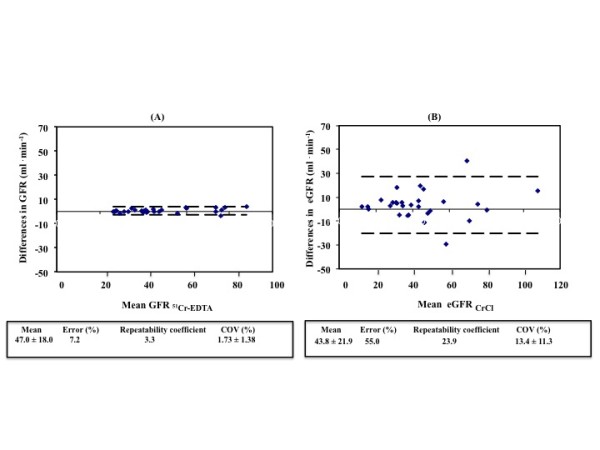
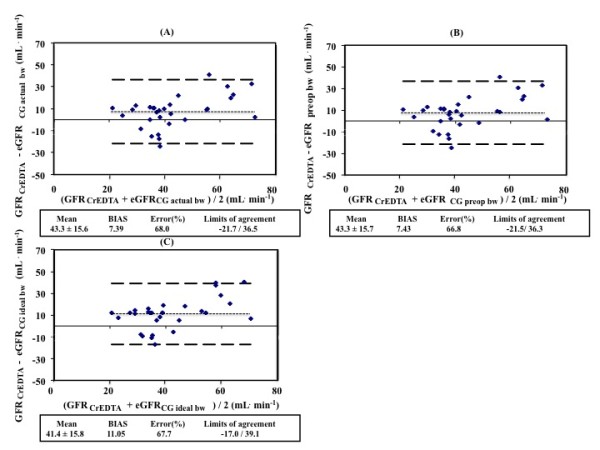
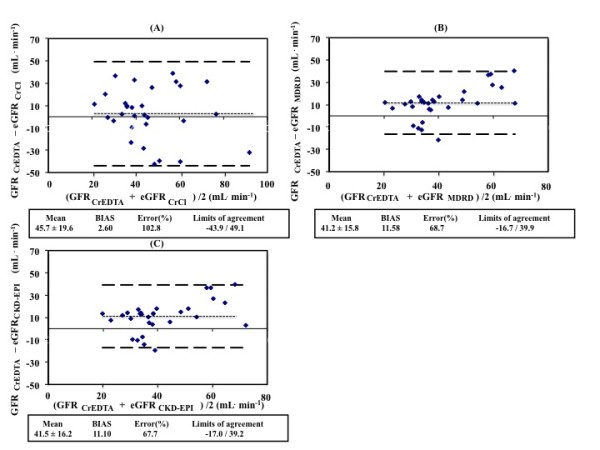
The within-group error was lower for GFR51Cr-EDTA than the urinary CrCl method, 7.2% versus 55.0%. The between-method bias was 2.6, 11.6, 11.1 and 7.39 ml/min for eGFRCrCl, eGFRMDRD, eGFRCKD-EPI and eGFRCG, respectively, when compared to GFR51Cr-EDTA. The error was 103%, 68.7%, 67.7% and 68.0% for eGFRCrCl, eGFRMDRD, eGFRCKD-EPI and eGFRCG, respectively, when compared to GFR51Cr-EDTA.
The study demonstrated poor precision of the commonly utilized urinary CrCl method for assessment of GFR in critically ill patients with early AKI, suggesting that this should not be used as a reference method when validating new methods for assessing kidney function in this patient population. The commonly used estimating equations perform poorly when estimating GFR, with high biases and unacceptably high errors.
在急性肾损伤(AKI)的危重症患者中,估算肾功能对于合理用药和调整治疗策略很重要,但由于肾功能、肌酐代谢和液体平衡的波动,这具有挑战性。目前缺乏关于早期AKI中评估肾小球滤过率(GFR)的估算方法与金标准方法之间一致性的数据。我们评估了尿肌酐清除率(CrCl)与三个常用估算方程,即Cockcroft Gault(CG)方程、肾脏病饮食改良(MDRD)方程和慢性肾脏病流行病学协作组(CKD-EPI)方程,与通过铬-乙二胺四乙酸(51Cr-EDTA)输注清除率测量的GFR相比,在心脏手术复杂后的早期AKI危重症患者中的一致性。
对30例早期AKI患者在重症监护病房进行研究,时间为心脏手术复杂后的2至12天。通过公式计算51Cr-EDTA的输注清除率作为GFR(GFR51Cr-EDTA)的测量值:GFR(mL/min/1.73m2)=(51Cr-EDTA输注速率×1.73)/(动脉血51Cr-EDTA×体表面积),并与尿CrCl以及三个估算方程得出的估算GFR(eGFR)进行比较。在两个30分钟时间段收集尿液以测量尿流率和尿肌酐。尿CrCl通过公式计算:CrCl(mL/min/1.73m2)=(尿量×尿肌酐×1.73)/(血清肌酐×30分钟×体表面积)。
GFR51Cr-EDTA的组内误差低于尿CrCl方法,分别为7.2%和55.0%。与GFR51Cr-EDTA相比,eGFRCrCl、eGFRMDRD、eGFRCKD-EPI和eGFRCG的方法间偏差分别为2.6、11.6、11.1和7.39 ml/min。与GFR51Cr-EDTA相比,eGFRCrCl、eGFRMDRD、eGFRCKD-EPI和eGFRCG的误差分别为103%、68.7%、67.7%和68.0%。
该研究表明,在早期AKI危重症患者中,常用的尿CrCl方法评估GFR的精度较差,这表明在验证该患者群体肾功能评估新方法时,不应将其用作参考方法。常用的估算方程在估算GFR时表现不佳,偏差高且误差高得令人无法接受。