Deng Kai, Zhu Hong, Chen Mo, Wu Junchao, Hu Renwei, Tang Chengwei
Department of Gastroenterology, West China Hospital, Sichuan University, Chengdu, 610041, China.
Department of Abdominal Cancer, West China Hospital, Sichuan University, Chengdu, 610041, China.
PLoS One. 2016 Mar 17;11(3):e0151608. doi: 10.1371/journal.pone.0151608. eCollection 2016.
Accurately distinguishing serosal invasion in patients with gastric cancer (GC) prior to surgery can be difficult. Molecular analysis of peritoneal fluid (MAPF) for free cancer cells with higher sensitivity than other methods; however, its prognostic value for GC remains controversial, precluding its application in clinical practice.
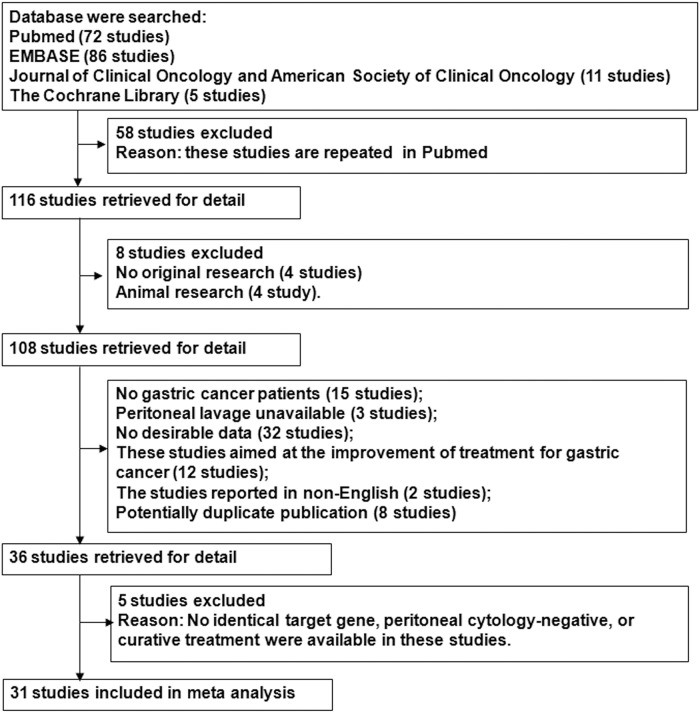
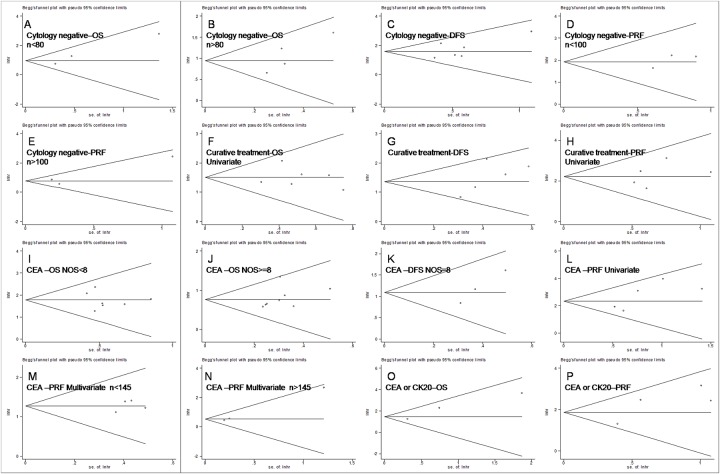
PubMed, EMBASE and other databases were systematically searched. Thirty-one studies were eligible for the meta-analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were pooled for overall survival (OS), disease-free survival (DFS) and peritoneal recurrence-free survival (PRF).
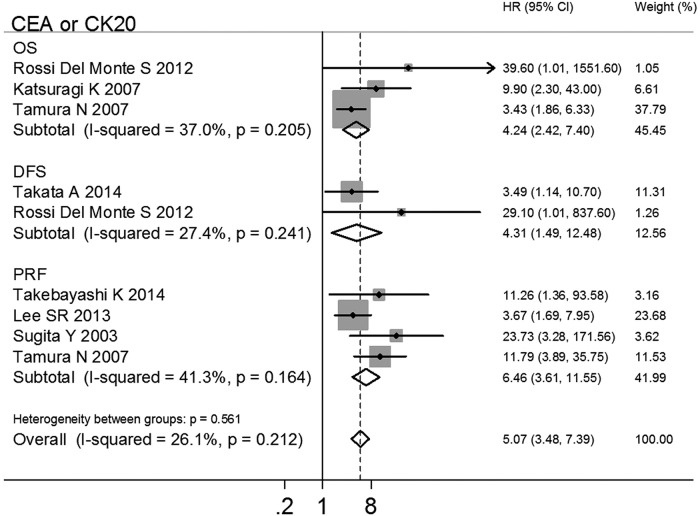
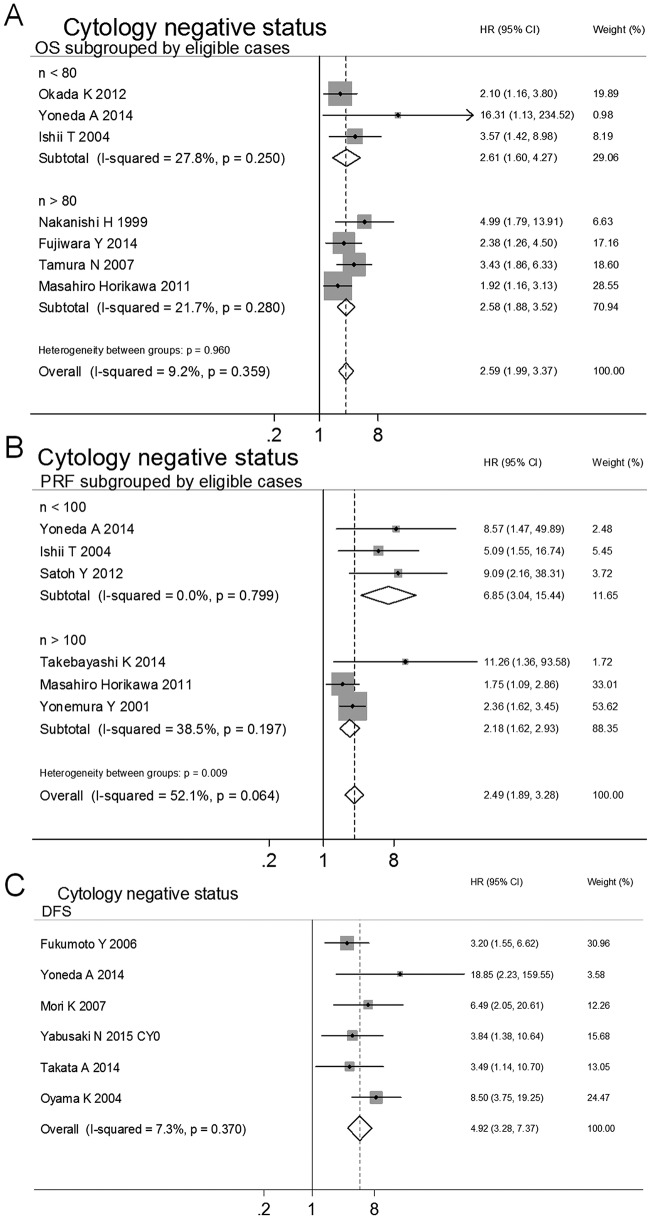
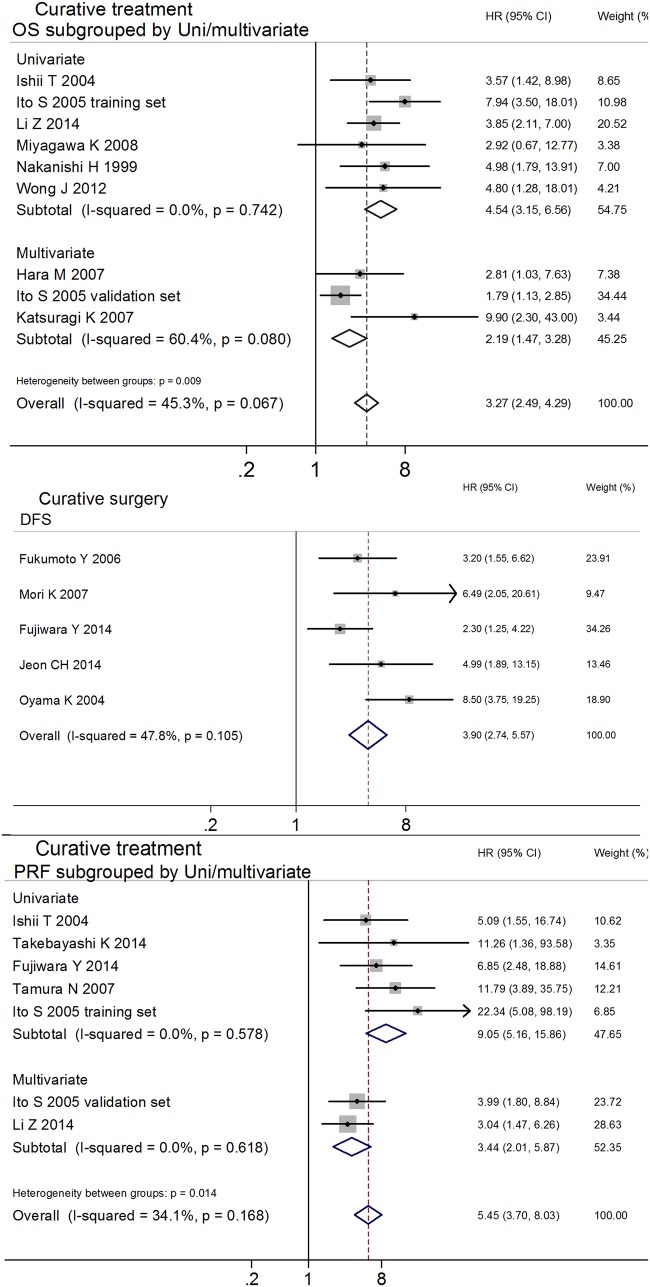
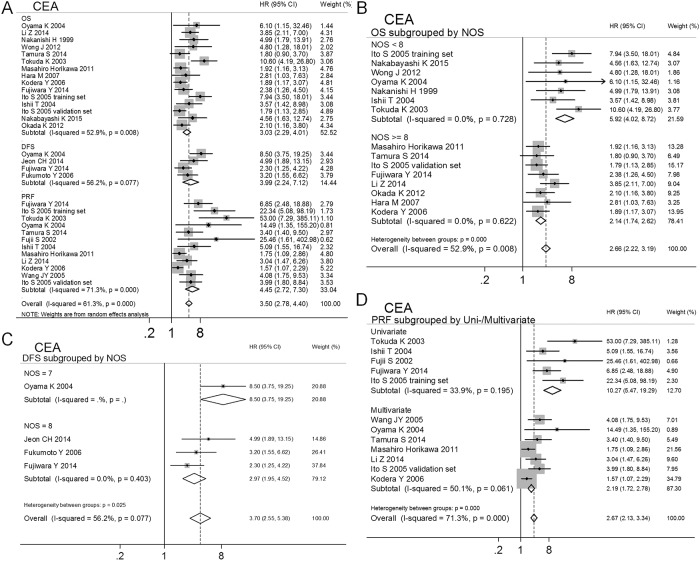
The current meta-analysis focused on patients with GC and negative cytological diagnoses. The results showed that positive MAPF status (MAPF+) led to poorer prognoses for OS (HR 2.59, 95% CI 1.99-3.37), DFS (HR 4.92, 95% CI 3.28-7.37) and PRF (HR 2.81, 95% CI 2.12-3.72) compared with negative MAPF status (MAPF-). Moreover, among the patients with GC who received curative treatment, the MAPF+ patients had poorer prognoses for OS (HR 3.27, 95% CI 2.49-4.29), DFS (HR 3.90, 95% CI 2.74-5.57) and PRF (HR 5.45, 95% CI 3.70-8.03). A meta-analysis of multivariate-adjusted HRs demonstrated that MAPF+ status was an independent prognostic factor for patients with GC who underwent curative treatment (OS: HR 2.19, 95% CI 1.47-3.28; PRF: HR 3.44, 95% CI 2.01-5.87). Using the identical target genes (CEA, CEA/CK20) as molecular markers, the patients with GC who were MAPF+ had significantly worse prognoses for OS (CEA: HR 3.03, 95% CI 2.29-4.01; CEA/CK20: HR 4.24, 95% CI 2.42-7.40), DFS (CEA: HR 3.99, 95% CI 2.24-7.12; CEA/CK20: HR 4.31, 95% CI 1.49-2.48) and PRF (CEA: HR 4.45, 95% CI 2.72-7.31; CEA/CK20: HR 6.46, 95% CI 3.62-11.55) than the patients who were MAPF-.
CONCLUSION/SIGNIFICANCE: The above results demonstrate that MAPF could be a prognostic indicator for patients with GC who have a negative cytological diagnosis and/or are receiving curative treatment. MAPF could provide clinicians with additional prognostic information that could aid in developing individualized treatment plans prior to surgery. The widely used target genes CEA, CEA/CK20 were confirmed to be valuable MAPF markers for predicting the prognosis of GC.
术前准确区分胃癌(GC)患者的浆膜侵犯可能具有挑战性。对腹腔积液进行分子分析(MAPF)以检测游离癌细胞,其敏感性高于其他方法;然而,其对GC的预后价值仍存在争议,这阻碍了其在临床实践中的应用。
系统检索了PubMed、EMBASE和其他数据库。31项研究符合荟萃分析的条件。汇总总生存期(OS)、无病生存期(DFS)和无腹膜复发生存期(PRF)的风险比(HRs)及95%置信区间(CIs)。
当前的荟萃分析聚焦于细胞学诊断为阴性的GC患者。结果显示,与MAPF阴性(MAPF-)状态相比,MAPF阳性(MAPF+)状态导致OS(HR 2.59,95% CI 1.99 - 3.37)、DFS(HR 4.92,95% CI 3.28 - 7.37)和PRF(HR 2.81,95% CI 2.12 - 3.72)的预后更差。此外,在接受根治性治疗的GC患者中,MAPF+患者的OS(HR 3.27,95% CI 2.49 - 4.29)、DFS(HR 3.90,95% CI 2.74 - 5.57)和PRF(HR 5.45,95% CI 3.70 - 8.03)预后更差。多变量调整后的HRs荟萃分析表明,MAPF+状态是接受根治性治疗的GC患者的独立预后因素(OS:HR 2.19,95% CI 1.47 - 3.28;PRF:HR 3.44,95% CI 2.01 - 5.87)。使用相同的靶基因(CEA、CEA/CK20)作为分子标志物,MAPF+的GC患者在OS(CEA:HR 3.03,95% CI 2.29 - 4.01;CEA/CK20:HR 4.24,95% CI 2.42 - 7.40)、DFS(CEA:HR 3.99,95% CI 2.24 - 7.12;CEA/CK20:HR 4.31,95% CI 1.49 - 2.48)和PRF(CEA:HR 4.45,95% CI 2.72 - 7.31;CEA/CK20:HR 6.46,95% CI 3.62 - 11.55)方面的预后明显比MAPF-患者差。
结论/意义:上述结果表明,MAPF可能是细胞学诊断为阴性和/或接受根治性治疗的GC患者的预后指标。MAPF可为临床医生提供额外的预后信息,有助于在手术前制定个体化治疗方案。广泛使用的靶基因CEA、CEA/CK20被证实是预测GC预后的有价值的MAPF标志物。