Terrin Gianluca, Conte Francesca, Scipione Antonella, Aleandri Vincenzo, Di Chiara Maria, Bacchio Erica, Messina Francesco, De Curtis Mario
Department of Gynecology-Obstetrics and Perinatal Medicine, "Sapienza" University of Rome, Viale del Policlinico 155, 00161, Rome, Italy.
Department of Pediatrics, "Sapienza" University of Rome, Viale del Policlinico 155, Rome, 00161, Italy.
BMC Pregnancy Childbirth. 2016 Mar 23;16:63. doi: 10.1186/s12884-016-0849-4.
A multidisciplinary committee composed of a panel of experts, including a member of the American Academy of Pediatrics and American Institute of Architects, has suggested that the delivery room (DR) and the neonatal intensive care units (NICU) room should be directly interconnected. We aimed to investigate the impact of the architectural design of the DR and the NICU on neonatal outcome.
Two cohorts of preterm neonates born at < 32 weeks of gestational age, consecutively observed during 2 years, were compared prospectively before (Cohort 1: "conventional DR") and after architectural renovation of the DR realized in accordance with specific standards (Cohort 2: "new concept of DR"). In Cohort 1, neonates were initially cared for a conventional resuscitation area, situated in the DR, and then transferred to the NICU, located on a separate floor of the same hospital. In Cohort 2 neonates were assisted at birth directly in the NICU room, which was directly connected to the DR via a pass-through door. The primary outcome of the study was morbidity, defined by the proportion of neonates with at least one complication of prematurity (i.e., late-onset sepsis, patent ductus arteriosus, intraventricular hemorrhage, periventricular leukomalacia, bronchopulmonary dysplasia, retinopathy of prematurity and necrotizing enterocolitis). Secondary outcomes were mortality and duration of hospitalization. Statistical analysis was performed using standard methods by SPSS software.
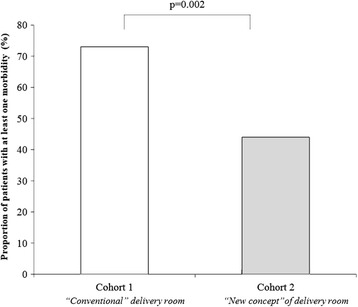
We enrolled 106 neonates (56 in Cohort 1 and 50 in Cohort 2). The main clinical and demographic characteristics of the 2 cohorts were similar. Moderate hypothermia (body temperature ≤ 35.9 °C) was more frequent in Cohort 1 (57%) compared with Cohort 2 (24%, p = 0.001). Morbidity was increased in Cohort 1 (73%) compared with Cohort 2 (44%, p = 0.002). No statistically significant differences in mortality and median duration of hospitalization were observed between the 2 cohorts of the study.
If realized according to the proposed architectural standards, renovation of DR and NICU may represent an opportunity to reduce morbidity in preterm neonates.
一个由专家组成的多学科委员会,其中包括美国儿科学会和美国建筑师协会的成员,建议产房(DR)和新生儿重症监护病房(NICU)应直接相连。我们旨在研究产房和新生儿重症监护病房的建筑设计对新生儿结局的影响。
前瞻性比较了两组胎龄小于32周的早产儿,这两组是在2年期间连续观察的,一组是在产房按照特定标准进行建筑翻新之前(队列1:“传统产房”),另一组是在翻新之后(队列2:“产房新概念”)。在队列1中,新生儿最初在位于产房的传统复苏区域接受护理,然后转移到位于同一家医院不同楼层的新生儿重症监护病房。在队列2中,新生儿出生时直接在新生儿重症监护病房内得到协助,该病房通过一扇传递门与产房直接相连。该研究的主要结局是发病率,定义为至少有一种早产并发症(即晚发性败血症、动脉导管未闭、脑室内出血、脑室周围白质软化、支气管肺发育不良、早产儿视网膜病变和坏死性小肠结肠炎)的新生儿比例。次要结局是死亡率和住院时间。使用SPSS软件通过标准方法进行统计分析。
我们纳入了106例新生儿(队列1中有56例,队列2中有50例)。两组的主要临床和人口统计学特征相似。与队列2(24%,p = 0.001)相比,队列1中中度低温(体温≤35.9°C)更为常见(57%)。与队列2(44%,p = 0.002)相比,队列1中的发病率更高(73%)。在该研究的两组之间,未观察到死亡率和住院中位时间的统计学显著差异。
如果按照提议的建筑标准进行翻新,产房和新生儿重症监护病房的改造可能是降低早产儿发病率的一个机会。