Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Washington2Hutchinson Institute for Cancer Outcomes Research, Fred Hutchinson Cancer Research Center, Seattle, Washington3Pharmaceutical Outcomes Research and Policy Prog.
Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Washington.
JAMA Oncol. 2016 Jul 1;2(7):890-8. doi: 10.1001/jamaoncol.2015.6275.
Prostate-specific antigen (PSA) screening for prostate cancer is controversial. Experts have suggested more personalized or more conservative strategies to improve benefit-risk tradeoffs, but the value of these strategies-particularly when combined with increased conservative management for low-risk cases-is uncertain.
To evaluate the potential cost-effectiveness of plausible PSA screening strategies and to assess the value added by increased use of conservative management among low-risk, screen-detected cases.
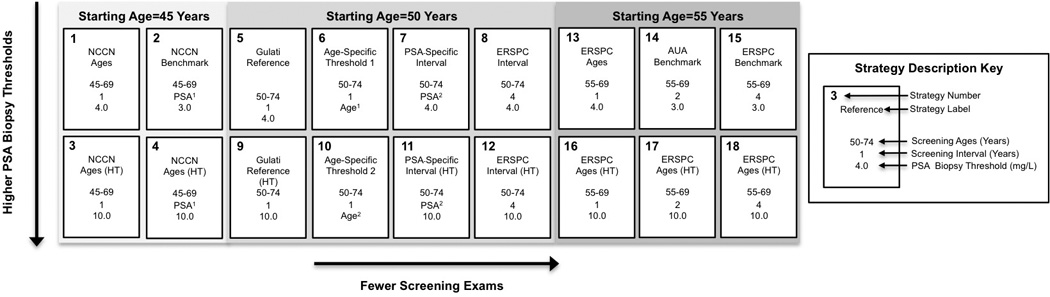
DESIGN, SETTING, AND PARTICIPANTS: A microsimulation model of prostate cancer incidence and mortality was created. A simulated contemporary cohort of US men beginning at 40 years of age underwent 18 strategies for PSA screening. Treatment strategies included (1) contemporary treatment practices based on age and cancer stage and grade observed in the Surveillance, Epidemiology, and End Results program in 2010 or (2) selective treatment practices whereby cases with a Gleason score lower than 7 and clinical T2a stage cancer or lower are treated only after clinical progression, and all other cases undergo contemporary treatment practices. National and trial data on PSA growth, screening and biopsy patterns, incidence of prostate cancer, treatment distributions, treatment efficacy, mortality, health-related quality of life, and direct medical expenditure were analyzed. Data were collected from March 18, 2009, to August 15, 2014, and analyzed from November 20, 2012, to December 11, 2015.
Eighteen screening strategies that vary by start and stop age, screening interval, and criteria for biopsy referral and contemporary or selective treatment practices.
Life-years (LYs), quality-adjusted life-years (QALYs), direct medical expenditure, and cost per LY and QALY gained.
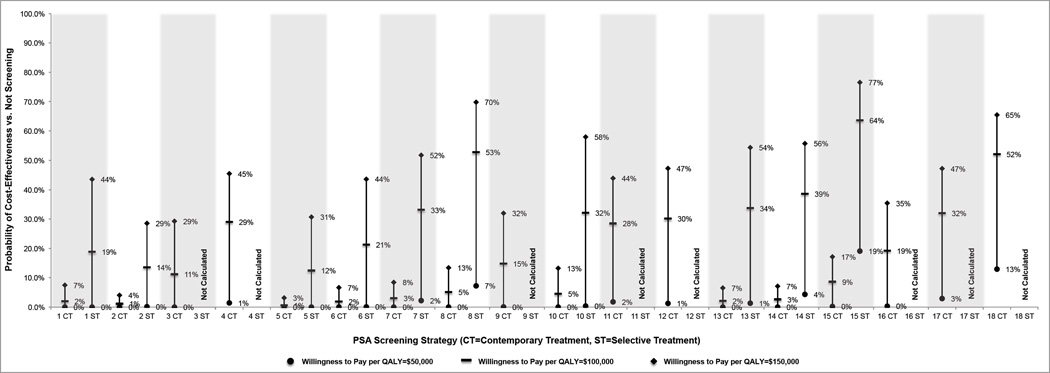
All 18 screening strategies were associated with increased LYs (range, 0.03-0.06) and costs ($263-$1371) compared with no screening, with the cost ranging from $7335 to $21 649 per LY. With contemporary treatment, only strategies with biopsy referral for PSA levels higher than 10.0 ng/mL or age-dependent thresholds were associated with increased QALYs (0.002-0.004), and only quadrennial screening of patients aged 55 to 69 years was potentially cost-effective in terms of cost per QALY (incremental cost-effectiveness ratio, $92 446). With selective treatment, all strategies were associated with increased QALYs (0.002-0.004), and several strategies were potentially cost-effective in terms of cost per QALY (incremental cost-effectiveness ratio, $70 831-$136 332).
For PSA screening to be cost-effective, it needs to be used conservatively and ideally in combination with a conservative management approach for low-risk disease.
前列腺特异性抗原(PSA)筛查前列腺癌存在争议。专家建议采用更个性化或更保守的策略来改善获益风险的权衡,但这些策略的价值,尤其是当与低危病例的更保守管理相结合时,尚不确定。
评估合理 PSA 筛查策略的潜在成本效益,并评估增加低危、筛查发现病例的保守管理的附加值。
设计、地点和参与者:建立了前列腺癌发病率和死亡率的微模拟模型。一个模拟的美国 40 岁以上男性的当代队列接受了 18 种 PSA 筛查策略。治疗策略包括(1)根据 2010 年监测、流行病学和最终结果计划中观察到的年龄和癌症阶段和分级的当代治疗实践,或(2)选择性治疗实践,即只有 Gleason 评分低于 7 且临床 T2a 期癌症或更低的病例才在临床进展后进行治疗,而所有其他病例则采用当代治疗实践。分析了全国和试验中关于 PSA 增长、筛查和活检模式、前列腺癌发病率、治疗分布、治疗效果、死亡率、健康相关生活质量和直接医疗支出的数据。数据收集于 2009 年 3 月 18 日至 2014 年 8 月 15 日,并于 2012 年 11 月 20 日至 2015 年 12 月 11 日进行分析。
18 种筛查策略,根据起始和停止年龄、筛查间隔和活检转诊标准以及当代或选择性治疗实践而有所不同。
寿命年(LYs)、质量调整寿命年(QALYs)、直接医疗支出以及每 LY 和 QALY 获得的成本。
与不筛查相比,所有 18 种筛查策略都与 LYs 的增加(范围为 0.03-0.06)和成本(263-1371 美元)相关,每 LY 的成本为 7335-21649 美元。采用当代治疗方法,只有 PSA 水平高于 10.0ng/mL 或年龄相关阈值的活检转诊策略与 QALYs 的增加(0.002-0.004)相关,并且只有 55-69 岁患者的每 4 年一次筛查在每 QALY 的成本方面具有成本效益(增量成本效益比,92446 美元)。采用选择性治疗方法,所有策略均与 QALYs 的增加(0.002-0.004)相关,并且在每 QALY 的成本方面(增量成本效益比,70831-136332 美元),有几种策略具有成本效益。
为了使 PSA 筛查具有成本效益,需要对其进行保守应用,理想情况下与低危疾病的保守管理方法相结合。