Matsuda Dean K, Bharam Srino, White Brian J, Matsuda Nicole A, Safran Marc
1. DISC Sports and Spine Center, 13160 Mindanao Way, Suite 300, Marina del Rey, CA 90292, USA.
2. 130 E 77th St, New York, NY 10075, USA.
J Hip Preserv Surg. 2015 Jan 29;2(1):56-64. doi: 10.1093/jhps/hnv001. eCollection 2015 Jan.
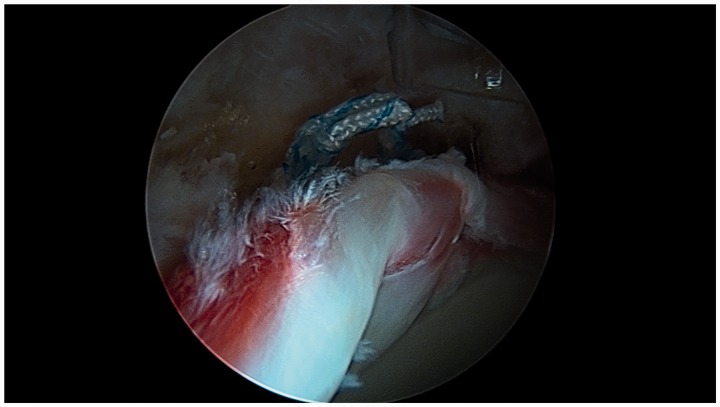
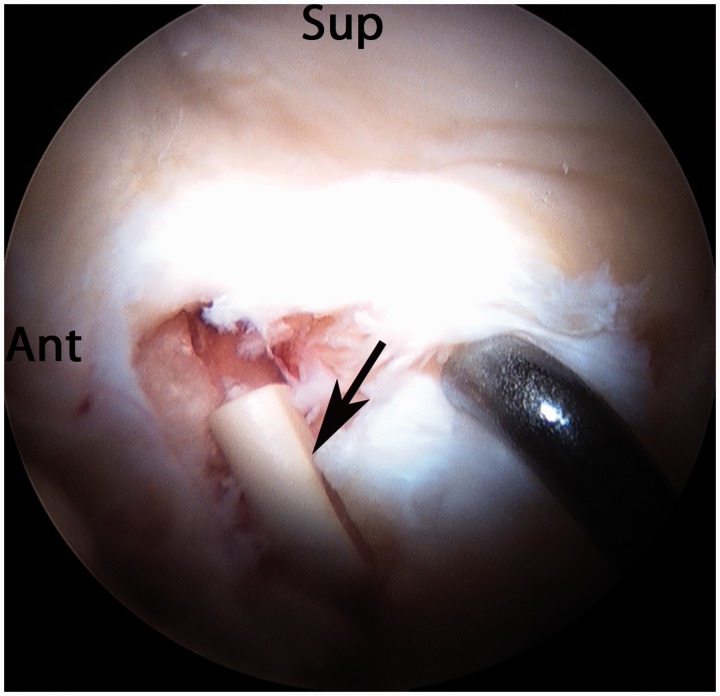
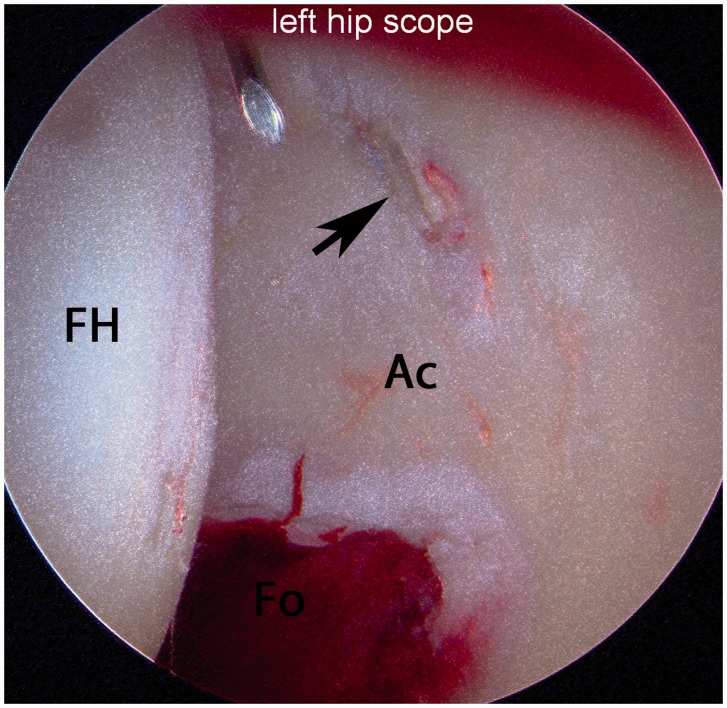
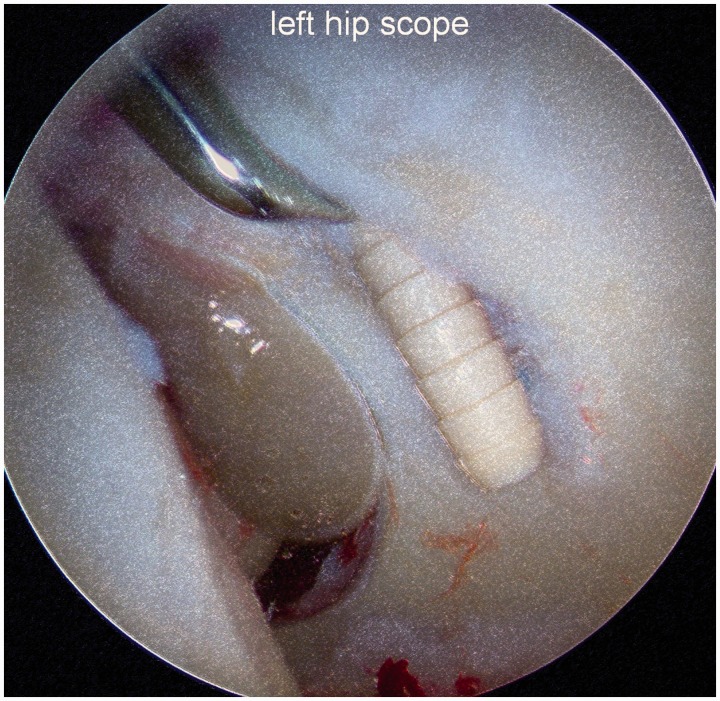
The purpose of this study is to investigate the outcomes from anchor-induced chondral damage of the hip, both with and without frank chondral penetration. A multicenter retrospective case series was performed of patients with chondral deformation or penetration during initial hip arthroscopic surgery. Intra-operative findings, post-surgical clinical courses, hip outcome scores and descriptions of arthroscopic treatment in cases requiring revision surgery and anchor removal are reported. Five patients (three females) of mean age 32 years (range, 16-41 years) had documented anchor-induced chondral damage with mean 3.5 years (range, 1.5-6.0 years) follow-up. The 1 o'clock position (four cases) and anterior and mid-anterior portals (two cases each) were most commonly implicated. Two cases of anchor-induced acetabular chondral deformation without frank penetration had successful clinical and radiographic outcomes, while one case progressed from deformation to chondral penetration with clinical worsening. Of the cases that underwent revision hip arthroscopy, all three had confirmed exposed hard anchors which were removed. Two patients have had clinical improvement and one patient underwent early total hip arthroplasty. Anchor-induced chondral deformation without frank chondral penetration may be treated with close clinical and radiographic monitoring with a low threshold for revision surgery and anchor removal. Chondral penetration should be treated with immediate removal of offending hard anchor implants. Preventative measures include distal-based portals, small diameter and short anchors, removable hard anchors, soft suture-based anchors, curved drill and anchor insertion instrumentation and attention to safe trajectories while visualizing the acetabular articular surface.
本研究的目的是调查髋部锚钉引起的软骨损伤的结果,包括有无明显软骨穿透的情况。对初次髋关节镜手术期间发生软骨变形或穿透的患者进行了一项多中心回顾性病例系列研究。报告了术中发现、术后临床病程、髋关节结局评分以及需要翻修手术和取出锚钉的病例的关节镜治疗描述。5例患者(3例女性),平均年龄32岁(范围16 - 41岁),记录有锚钉引起的软骨损伤,平均随访3.5年(范围1.5 - 6.0年)。最常涉及的部位是1点位置(4例)以及前侧和前中侧入路(各2例)。2例锚钉引起的髋臼软骨变形但无明显穿透的患者获得了成功的临床和影像学结果,而1例从变形发展为软骨穿透,临床症状恶化。在接受翻修髋关节镜检查的病例中,所有3例均证实有暴露的硬锚钉并予以取出。2例患者临床症状改善,1例患者早期接受了全髋关节置换术。对于锚钉引起的无明显软骨穿透的软骨变形,可通过密切的临床和影像学监测进行治疗,翻修手术和取出锚钉的阈值较低。软骨穿透应立即取出引起问题的硬锚钉植入物。预防措施包括基于远端的入路、小直径和短锚钉、可取出的硬锚钉、基于软缝线的锚钉、弯曲的钻头和锚钉插入器械,以及在可视化髋臼关节面时注意安全轨迹。