Foster Josh, Mauger Alexis, Thomasson Katie, White Stephanie, Taylor Lee
Applied Sport and Exercise Physiology Research Group, Institute of Sport and Physical Activity Research, Department of Sport Science and Physical Activity, University of Bedfordshire Bedfordshire, UK.
Endurance Research Group, School of Sport and Exercise Sciences, University of Kent Chatham, UK.
Front Pharmacol. 2016 Mar 14;7:54. doi: 10.3389/fphar.2016.00054. eCollection 2016.
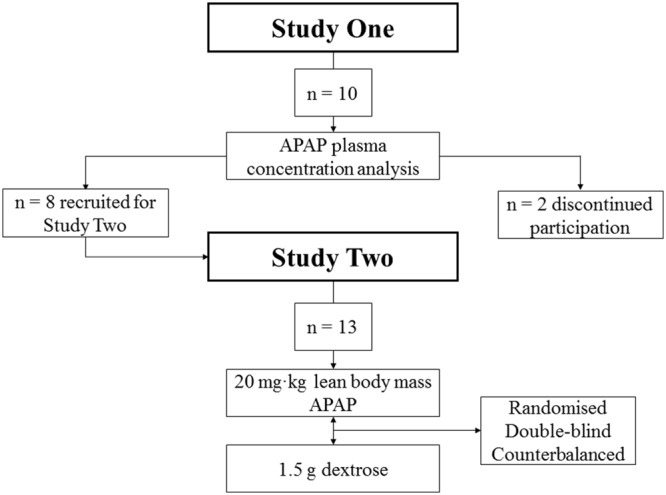
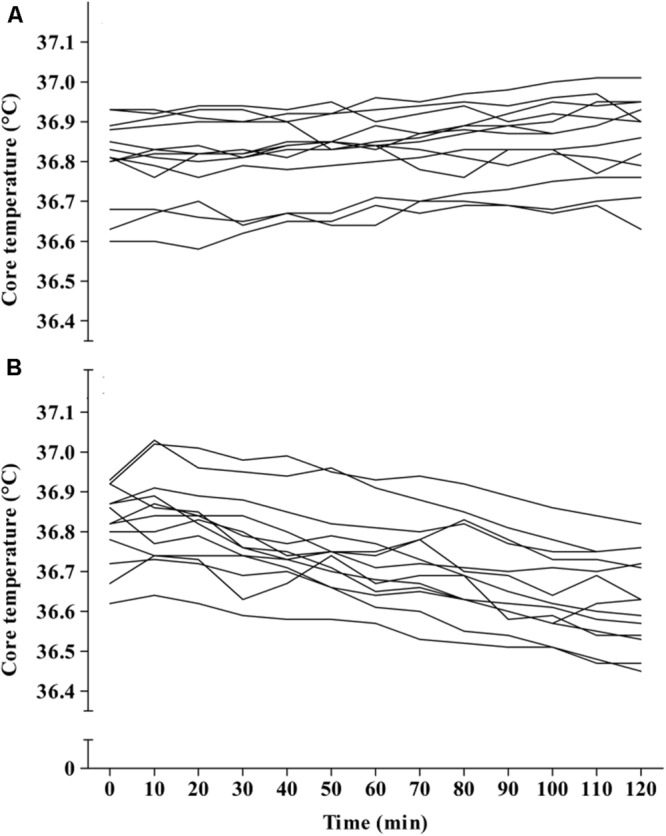
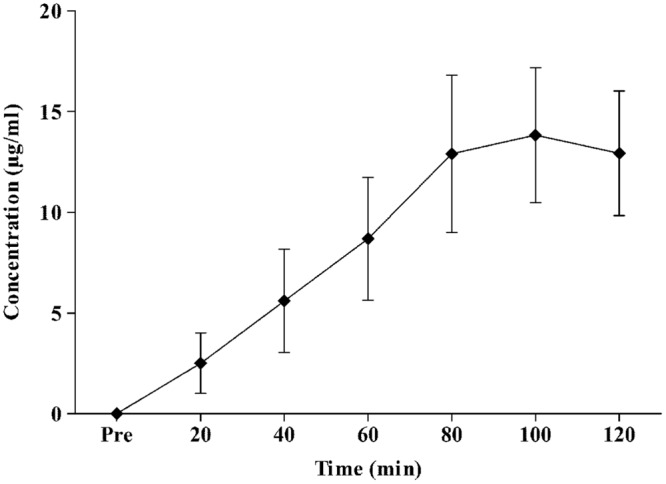
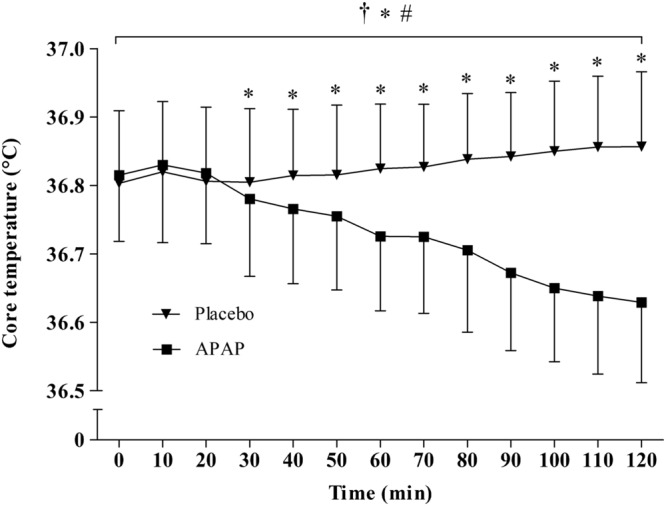
In non-febrile mouse models, high dose acetaminophen administration causes profound hypothermia. However, this potentially hazardous side-effect has not been confirmed in non-febrile humans. Thus, we sought to ascertain whether an acute therapeutic dose (20 mg⋅kg lean body mass) of acetaminophen would reduce non-febrile human core temperature in a sub-neutral environment. Ten apparently healthy (normal core temperature, no musculoskeletal injury, no evidence of acute illness) Caucasian males participated in a preliminary study (Study 1) to determine plasma acetaminophen concentration following oral ingestion of 20 mg⋅kg lean body mass acetaminophen. Plasma samples (every 20 min up to 2-hours post ingestion) were analyzed via enzyme linked immunosorbent assay. Thirteen (eight recruited from Study 1) apparently healthy Caucasian males participated in Study 2, and were passively exposed to 20°C, 40% r.h. for 120 min on two occasions in a randomized, repeated measures, crossover design. In a double blind manner, participants ingested acetaminophen (20 mg⋅kg lean body mass) or a placebo (dextrose) immediately prior to entering the environmental chamber. Rectal temperature, skin temperature, heart rate, and thermal sensation were monitored continuously and recorded every 10 min. In Study 1, the peak concentration of acetaminophen (14 ± 4 μg/ml) in plasma arose between 80 and 100 min following oral ingestion. In Study 2, acetaminophen ingestion reduced the core temperature of all participants, whereas there was no significant change in core temperature over time in the placebo trial. Mean core temperature was significantly lower in the acetaminophen trial compared with that of a placebo (p < 0.05). The peak reduction in core temperature in the acetaminophen trial was reached at 120 min in six of the thirteen participants, and ranged from 0.1 to 0.39°C (average peak reduction from baseline = 0.19 ± 0.09°C). There was no significant difference in skin temperature, heart rate, or thermal sensation between the acetaminophen and placebo trials (p > 0.05). The results indicate oral acetaminophen reduces core temperature of humans exposed to an environment beneath the thermal neutral zone. These results suggest that acetaminophen may inhibit the thermogenic mechanisms required to regulate core temperature during exposure to sub-neutral environments.
在无发热的小鼠模型中,高剂量给予对乙酰氨基酚会导致深度体温过低。然而,这种潜在的有害副作用在无发热的人类中尚未得到证实。因此,我们试图确定对乙酰氨基酚的急性治疗剂量(20毫克·千克瘦体重)是否会在亚中性环境中降低无发热人类的核心体温。十名表面健康(核心体温正常、无肌肉骨骼损伤、无急性疾病迹象)的白人男性参与了一项初步研究(研究1),以确定口服20毫克·千克瘦体重对乙酰氨基酚后血浆中对乙酰氨基酚的浓度。通过酶联免疫吸附测定法分析血浆样本(摄入后每20分钟直至2小时)。十三名(八名从研究1招募)表面健康的白人男性参与了研究2,并在随机、重复测量、交叉设计中两次被动暴露于20°C、40%相对湿度环境120分钟。以双盲方式,参与者在进入环境舱前立即摄入对乙酰氨基酚(20毫克·千克瘦体重)或安慰剂(葡萄糖)。连续监测直肠温度、皮肤温度、心率和热感觉,并每10分钟记录一次。在研究1中,口服后80至100分钟血浆中对乙酰氨基酚的峰值浓度(14±4微克/毫升)出现。在研究2中,摄入对乙酰氨基酚降低了所有参与者 的核心体温,而在安慰剂试验中核心体温随时间没有显著变化。与安慰剂相比,对乙酰氨基酚试验中的平均核心体温显著更低(p<0.05)。在对乙酰氨基酚试验中,十三名参与者中有六名在120分钟时达到核心体温的最大降幅,范围为0.1至0.39°C(从基线的平均最大降幅=0.19±0.09°C)。对乙酰氨基酚试验和安慰剂试验之间的皮肤温度、心率或热感觉没有显著差异(p>0.05)。结果表明口服对乙酰氨基酚会降低暴露于热中性区以下环境的人类的核心体温。这些结果表明,对乙酰氨基酚可能会抑制在暴露于亚中性环境期间调节核心体温所需的产热机制。