Allergy Pediatric Unit, Pediatrics Department, Sandro Pertini Hospital , Rome , Italy.
NESMOS Department, Faculty of Medicine and Psychology, Pediatric Unit Sant'Andrea Hospital, "Sapienza" University , Rome , Italy.
Front Pediatr. 2016 Mar 8;4:16. doi: 10.3389/fped.2016.00016. eCollection 2016.
Poor asthma control can lead to exercise-induced bronchoconstriction (EIB), but the relationship between subjective disease control and EIB is unclear. No studies have compared asthma control test (ACT) scores of children with those of their parents regarding EIB. We assessed whether ACT scores predict the occurrence of EIB in two age groups. We also evaluated ACT scores and objective measures as explanatory variables for airway response to exercise.
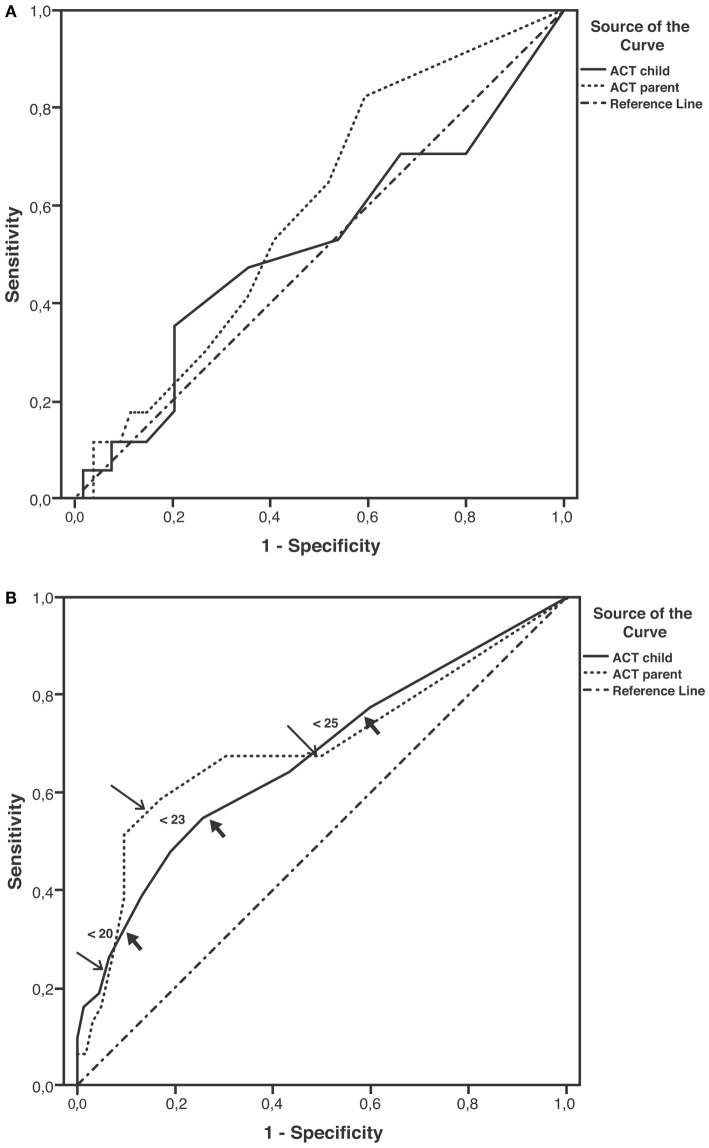
Patients (71, aged <12 years; 93, aged ≥12 years) and their parents completed an ACT questionnaire separately. Current therapy, skin prick testing, and spirometry at baseline and after exercise were assessed. EIB was defined as a fall in forced expiratory volume in 1 s (FEV1) of at least 12% from baseline. Sensitivity and specificity for cut-off values of ACT scores predictive of EIB were plotted, and the area under curve (AUC) was described.
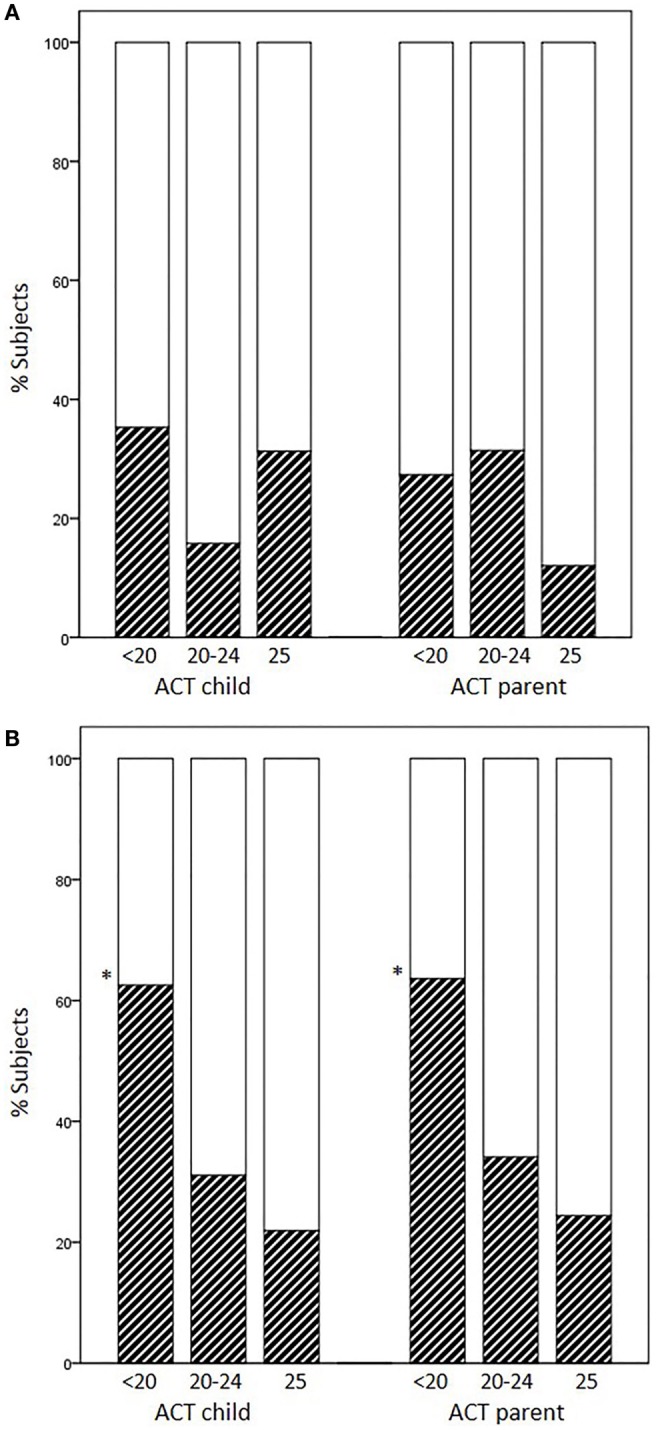
Atopy and current therapy were similarly frequent. EIB was observed in 23.9% of children aged <12 years and in 33.3% of children aged ≥12 years. EIB occurrence in subjects previously scored as having full control (25), partial control (20-24), and no control (<20) varied according to the age group and responders. Percentages of EIB cases increased as ACT scores decreased in children aged ≥12 years alone (child ACT scores, 25: 21.9%, 20-24: 31.1%, <20: 62.5%, p = 0.017). Plots for ACT scores as predictors of EIB yielded low non-significant AUC values in children aged <12 years; in contrast, moderate AUC values emerged in children aged ≥12 years (child: 0.67, p = 0.007; parent: 0.69, p = 0.002). Sensitivity of ACT scores below 20 as a predictor of EIB was low in older children (child: 32.3%, parent: 22.6%), whereas specificity was high (child: 90.3%, parent: 93.5%). Multiple regression analysis with percent fall in FEV1 as dependent variable included FEV1/FVC%, ACT child score, and gender in the prediction model (r = 0.42, p = 0.000).
ACT scores are a more effective means of excluding than confirming EIB in asthmatic patients aged ≥12 years; their predictive value decreases in younger patients. ACT scores together with lung function may help to predict airway response to exercise. New tools for pediatric asthma assessment may optimize this association.
哮喘控制不佳可导致运动诱发的支气管收缩(EIB),但主观疾病控制与 EIB 之间的关系尚不清楚。尚无研究比较过儿童和其父母的哮喘控制测试(ACT)评分与 EIB 之间的关系。我们评估了 ACT 评分是否可预测两个年龄组的 EIB 发生情况。我们还评估了 ACT 评分和客观测量值作为运动后气道反应的解释变量。
71 名年龄<12 岁的患者和 93 名年龄≥12 岁的患者及其父母分别完成了 ACT 问卷。在基线和运动后评估了当前治疗、皮肤点刺试验和肺量计检查。EIB 定义为用力呼气量 1 秒(FEV1)较基线下降至少 12%。绘制预测 EIB 的 ACT 评分截断值的敏感性和特异性曲线,并描述曲线下面积(AUC)。
变应原和当前治疗的发生率相似。年龄<12 岁的儿童中有 23.9%出现 EIB,年龄≥12 岁的儿童中有 33.3%出现 EIB。在之前评分显示完全控制(25)、部分控制(20-24)和无控制(<20)的受试者中,EIB 的发生率因年龄组和应答者而异。仅在年龄≥12 岁的儿童中,ACT 评分越低,EIB 病例的百分比越高(儿童 ACT 评分,25:21.9%,20-24:31.1%,<20:62.5%,p=0.017)。在年龄<12 岁的儿童中,ACT 评分作为 EIB 预测因子的 AUC 值较低且无统计学意义;相比之下,在年龄≥12 岁的儿童中,AUC 值适中(儿童:0.67,p=0.007;父母:0.69,p=0.002)。年龄较大的儿童中,ACT 评分<20 作为 EIB 预测因子的敏感性较低(儿童:32.3%,父母:22.6%),而特异性较高(儿童:90.3%,父母:93.5%)。以 FEV1 下降百分比为因变量的多元回归分析纳入了 FEV1/FVC%、儿童 ACT 评分和性别作为预测模型的变量(r=0.42,p=0.000)。
ACT 评分是一种更有效的方法,可排除≥12 岁哮喘患者的 EIB,而非确认 EIB;在年龄较小的患者中,其预测价值降低。ACT 评分与肺功能一起可帮助预测运动后的气道反应。评估儿童哮喘的新工具可能会优化这种关联。