Yan C H, Xu T, Zheng X Y, Sun J, Duan X L, Gu J L, Zhao C L, Zhu J, Wu Y H, Wu D P, Hu J D, Huang H, Jiang M, Li J, Hou M, Wang C, Shao Z H, Liu T, Hu Y, Huang X J
Peking University People's Hospital, Peking University Institute of Hematology, Beijing Key Laboratory of Hematopoietic Stem Cell Transplantation, Beijing 100044, China.
Zhonghua Xue Ye Xue Za Zhi. 2016 Mar;37(3):177-82. doi: 10.3760/cma.j.issn.0253-2727.2016.03.001.
To investigate the incidence, clinical and microbiological features of febrile, and risk factors during neutropenia periods in patients with hematological diseases.
From October 20, 2014 to March 20, 2015, consecutive patients who had hematological diseases and developed neutropenia during hospitalization were enrolled in the prospective, multicenter and observational study.
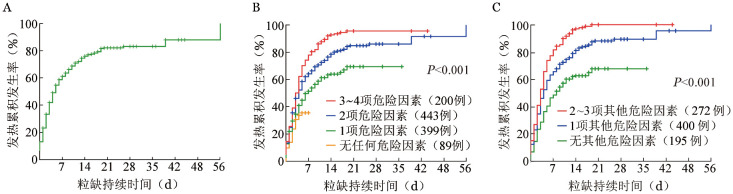
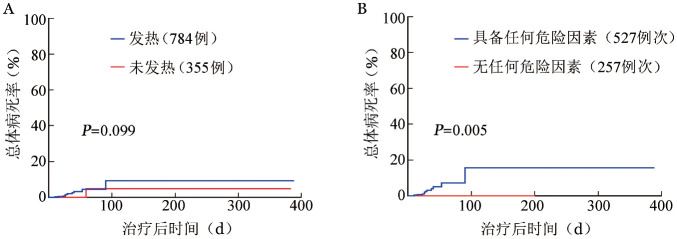
A total of 784 episodes of febrile occurred in 1 139 neutropenic patients with hematological diseases. The cumulative incidence of febrile was 81.9% at 21 days after neutropenia. Multivariate analysis suggested that central venous catheterization (P<0.001, HR=3.407, 95% CI 2.276-4.496), gastrointestinal mucositis (P<0.001, HR=10.548, 95% CI 3.245-28.576), previous exposure to broad-spectrum antibiotics within 90 days (P<0.001, HR=3.582, 95% CI 2.387-5.770) and duration of neutropenia >7 days (P<0.001,HR=4.194, 95% CI 2.572-5.618) were correlated with higher incidence of febrile during neutropenia. With the increase of the risk factors, the incidence of febrile increased gradually (35.4%, 69.2%, 86.1%, 95.6%, P<0.001). Of 784 febrile cases, 253 (32.3%) were unknown origin, 429 (54.7% )of clinical documented infections and 102(13.0%) of microbiological documented infections. The most common sites of infection were pulmonary (49.5%), upper respiratory (16.0%), crissum (9.8%), blood stream (7.7%). The most common pathogens were gram-negative bacteria (44.54%), followed by gram-positive bacteria (37.99% ) and fungi (17.47% ). There was no significant difference in mortality rates between cases with febrile and cases without febrile (9.2% vs 4.8%, P=0.099). Multivariate analysis also suggested that >40 years old (P=0.047, HR=5.000, 95% CI 0.853-28.013), hemodynamic instability (P=0.001, HR=13.185, 95% CI 2.983-54.915), prior colonization or infection by resistant pathogens (P=0.005, HR=28.734, 95% CI 2.921-313.744), blood stream infection (P=0.038, HR=9.715, 95% CI 1.110-81.969) and pulmonary infection (P=0.031, HR=25.905, 95% CI 1.381-507.006) were correlated with higher mortality rate in cases with febrile.
Febrile was the common complication during neutropenia periods in patients with hematological disease. There was different distribution of organisms in different sites of infection. Moreove, the duration of neutropenia >7 days, central venous catheterization, gastrointestinal mucositis and previous exposure to broad-spectrum antibiotics within 90 days were the risk factors for the higher incidence of febrile.
探讨血液系统疾病患者发热的发生率、临床及微生物学特征,以及中性粒细胞减少期的危险因素。
2014年10月20日至2015年3月20日,将住院期间发生中性粒细胞减少的血液系统疾病患者纳入前瞻性、多中心观察性研究。
1139例血液系统疾病中性粒细胞减少患者共发生784次发热。中性粒细胞减少后21天发热的累积发生率为81.9%。多因素分析表明,中心静脉置管(P<0.001,HR=3.407,95%CI 2.276-4.496)、胃肠道黏膜炎(P<0.001,HR=10.548,95%CI 3.245-28.576)、90天内曾使用过广谱抗生素(P<0.001,HR=3.582,95%CI 2.387-5.770)及中性粒细胞减少持续时间>7天(P<0.001,HR=4.194,95%CI 2.572-5.618)与中性粒细胞减少期发热发生率较高相关。随着危险因素数量的增加,发热发生率逐渐升高(35.4%、69.2%、86.1%、95.6%,P<0.001)。784例发热病例中,253例(32.3%)病因不明,429例(54.7%)为临床确诊感染,102例(13.0%)为微生物确诊感染。最常见的感染部位为肺部(49.5%)、上呼吸道(16.0%)、肛周(9.8%)、血流(7.7%)。最常见的病原体为革兰阴性菌(44.54%),其次为革兰阳性菌(37.99%)和真菌(17.47%)。发热患者与未发热患者的死亡率无显著差异(9.2%对4.8%,P=0.099)。多因素分析还表明,年龄>40岁(P=0.047,HR=5.000,95%CI 0.853-28.013)、血流动力学不稳定(P=0.001,HR=13.185,95%CI 2.983-54.915)、既往有耐药病原体定植或感染(P=0.005,HR=28.734,95%CI 2.921-313.744)、血流感染(P=0.038,HR=9.715,95%CI 1.110-81.969)及肺部感染(P=0.031,HR=25.905,95%CI 1.381-507.006)与发热患者较高的死亡率相关。
发热是血液系统疾病患者中性粒细胞减少期的常见并发症。不同感染部位的病原体分布不同。此外,中性粒细胞减少持续时间>7天、中心静脉置管、胃肠道黏膜炎及90天内曾使用过广谱抗生素是发热发生率较高的危险因素。