Okada Mari, Sato Mai, Ogura Masao, Kamei Koichi, Matsuoka Kentaro, Ito Shuichi
Division of Nephrology and Rheumatology, National Center for Child Health and Development, Tokyo, Japan.
Department of Pediatrics, Musashino Red Cross Hospital, 1-26-1 Kyonancho, Musashino, Tokyo, 180-8610, Japan.
BMC Res Notes. 2016 Mar 31;9:196. doi: 10.1186/s13104-016-1997-3.
Advances in long-term parenteral nutrition via indwelling central venous catheter have improved the quality of life and mortality in patients with life-threatening gastrointestinal diseases complicated with severely impaired absorption. However, infection to central venous catheter is still a common and critical complication for such patients. We encountered two patients under long-term parenteral nutrition who developed glomerulonephritis associated with central venous catheter infection. Persistent bacterial infection in indwelling medical devices placed in the blood-stream such as a ventricular-atrial shunt is known to cause glomerulonephritis, a condition termed shunt nephritis. We reported the clinical manifestations, treatment and their pathological findings in the two patients with glomerulonephritis associated with central venous catheter infection.
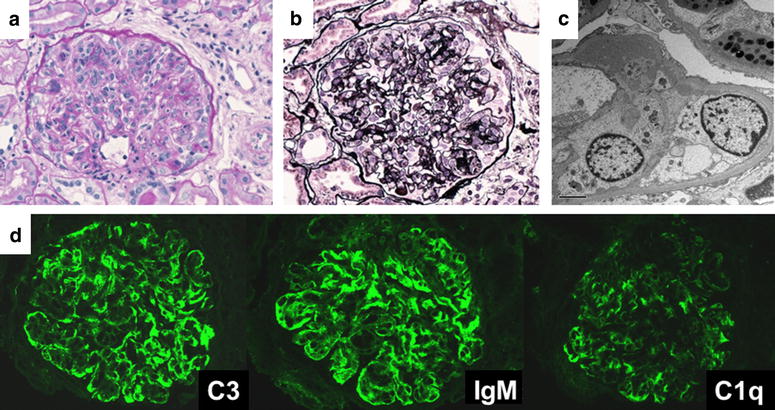
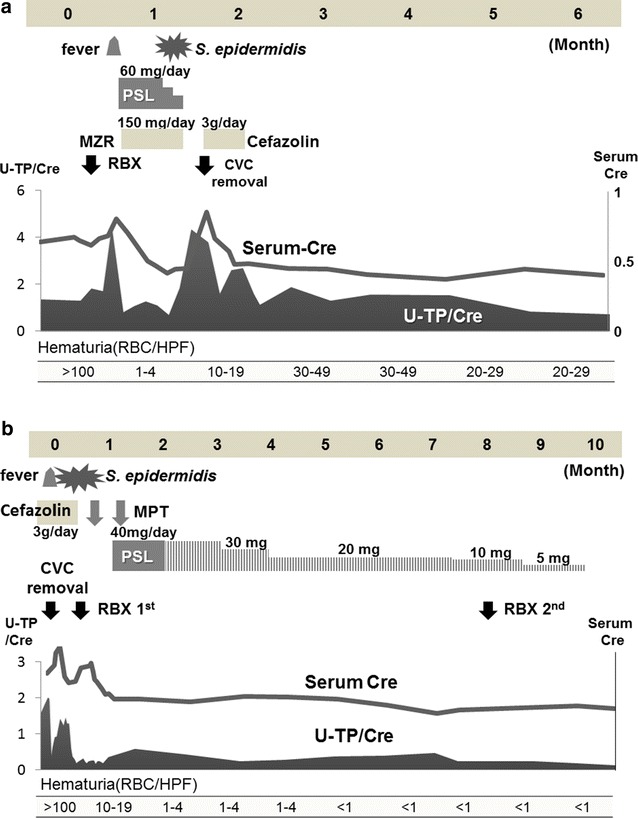
Both patients suffered from megacystis microcolon intestinal hypoperistalsis syndrome, a form of pseudo-Hirschsprung's disease. They had been receiving home parenteral nutrition via central venous catheter because of severe malabsorption. They presented proteinuria, hematuria, hypocomplementemia and positive PR3-antineutrophilic cytoplasmic antibody accompanied by Staphylococcus epidermidis infection in the central venous catheter. Their renal biopsy revealed membranoproliferative glomerulonephritis with positive C3 deposition. One of them recovered completely following the removal of catheter and administration of antibiotics, while another did not respond to the treatments. We then treated her with methylprednisolone pulse therapy followed by prednisolone. She responded well, and achieved complete remission.
As central venous catheter infection-related glomerulonephritis has a similar etiology to shunt nephritis, removal of the catheter and administration of antibiotics is fundamental to the treatment. If a patient is resistant to such conventional therapy, additional steroid and/or immunosuppressive agent could be considered. Although the number of patients with classical shunt nephritis is decreasing since the ventricular-peritoneal shunt has become became the major procedure for hydrocephalus, central venous catheter infection-related glomerulonephritis may increase in the future due to a marked increase in the number of patients receiving long-term parenteral nutrition. Routine urinalysis should be considered in such patients for early detection of central venous catheter infection-related glomerulonephritis.
通过留置中心静脉导管进行长期肠外营养的进展改善了患有危及生命的胃肠道疾病并伴有严重吸收障碍患者的生活质量和死亡率。然而,中心静脉导管感染仍是这类患者常见且严重的并发症。我们遇到了两名长期接受肠外营养的患者,他们发生了与中心静脉导管感染相关的肾小球肾炎。已知置于血流中的留置医疗装置(如脑室-心房分流管)中的持续性细菌感染会导致肾小球肾炎,即所谓的分流性肾炎。我们报告了这两名与中心静脉导管感染相关的肾小球肾炎患者的临床表现、治疗方法及其病理结果。
两名患者均患有巨膀胱小结肠肠蠕动不良综合征,这是一种假性先天性巨结肠病。由于严重吸收不良,他们一直通过中心静脉导管接受家庭肠外营养。他们出现蛋白尿、血尿、补体降低以及抗蛋白酶3-抗中性粒细胞胞浆抗体阳性,同时中心静脉导管伴有表皮葡萄球菌感染。他们的肾活检显示为伴有C3沉积阳性的膜增生性肾小球肾炎。其中一名患者在拔除导管并使用抗生素后完全康复,而另一名患者对治疗无反应。然后我们对她采用甲泼尼龙冲击疗法,随后使用泼尼松龙治疗。她反应良好,实现了完全缓解。
由于与中心静脉导管感染相关的肾小球肾炎与分流性肾炎病因相似,拔除导管并使用抗生素是治疗的基础。如果患者对这种传统治疗有抵抗性,可以考虑加用类固醇和/或免疫抑制剂。尽管自从脑室-腹腔分流术成为脑积水的主要手术方式后,典型分流性肾炎的患者数量在减少,但由于接受长期肠外营养的患者数量显著增加,未来与中心静脉导管感染相关的肾小球肾炎可能会增多。对于这类患者应考虑进行常规尿液分析,以便早期发现与中心静脉导管感染相关的肾小球肾炎。