Sabin Caroline A, Reiss Peter, Ryom Lene, Phillips Andrew N, Weber Rainer, Law Matthew, Fontas Eric, Mocroft Amanda, de Wit Stephane, Smith Colette, Dabis Francois, d'Arminio Monforte Antonella, El-Sadr Wafaa, Lundgren Jens D
Research Department of Infection and Population Health, University College London (UCL), Royal Free Campus, London, UK.
Academic Medical Center, Division of Infectious Diseases and Department of Global Health, University of Amsterdam, Amsterdam, The Netherlands.
BMC Med. 2016 Mar 31;14:61. doi: 10.1186/s12916-016-0588-4.
In March 2008, the D:A:D study published results demonstrating an increased risk of myocardial infarction (MI) for patients on abacavir (ABC). We describe changes to the use of ABC since this date, and investigate changes to the association between ABC and MI with subsequent follow-up.
A total of 49,717 D:A:D participants were followed from study entry until the first of an MI, death, 1 February 2013 or 6 months after last visit. Associations between a person's 10-year cardiovascular disease (CVD) risk and the likelihood of initiating or discontinuing ABC were assessed using multivariable logistic/Poisson regression. Poisson regression was used to assess the association between current ABC use and MI risk, adjusting for potential confounders, and a test of interaction was performed to assess whether the association had changed in the post-March 2008 period.
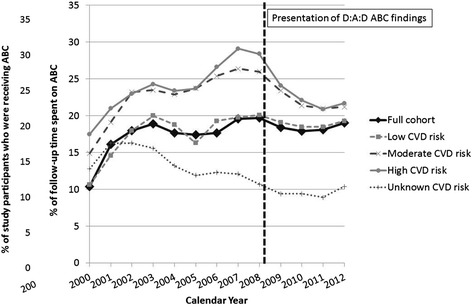
Use of ABC increased from 10 % of the cohort in 2000 to 20 % in 2008, before stabilising at 18-19 %. Increases in use pre-March 2008, and subsequent decreases, were greatest in those at moderate and high CVD risk. Post-March 2008, those on ABC at moderate/high CVD risk were more likely to discontinue ABC than those at low/unknown CVD risk, regardless of viral load (≤1,000 copies/ml: relative rate 1.49 [95 % confidence interval 1.34-1.65]; >1,000 copies/ml: 1.23 [1.02-1.48]); no such associations were seen pre-March 2008. There was some evidence that antiretroviral therapy (ART)-naïve persons at moderate/high CVD risk post-March 2008 were less likely to initiate ABC than those at low/unknown CVD risk (odds ratio 0.74 [0.48-1.13]). By 1 February 2013, 941 MI events had occurred in 367,559 person-years. Current ABC use was associated with a 98 % increase in MI rate (RR 1.98 [1.72-2.29]) with no difference in the pre- (1.97 [1.68-2.33]) or post- (1.97 [1.43-2.72]) March 2008 periods (interaction P = 0.74).
Despite a reduction in the channelling of ABC for patients at higher CVD risk since 2008, we continue to observe an association between ABC use and MI risk. Whilst confounding cannot be fully ruled out, this further diminishes channelling bias as an explanation for our findings.
2008年3月,D:A:D研究公布的结果显示,服用阿巴卡韦(ABC)的患者发生心肌梗死(MI)的风险增加。我们描述了自该日期以来ABC使用情况的变化,并通过后续随访调查ABC与MI之间关联的变化。
共有49717名D:A:D参与者从研究入组开始随访,直至首次发生MI、死亡、2013年2月1日或末次随访后6个月。使用多变量逻辑/泊松回归评估个体10年心血管疾病(CVD)风险与开始或停用ABC可能性之间的关联。使用泊松回归评估当前使用ABC与MI风险之间的关联,并对潜在混杂因素进行校正,同时进行交互作用检验以评估2008年3月之后这种关联是否发生了变化。
ABC的使用从2000年占队列的10%增加到2008年的20%,之后稳定在18% - 19%。2008年3月之前使用量的增加以及随后的减少,在CVD风险为中度和高度的人群中最为明显。2008年3月之后,CVD风险为中度/高度的ABC使用者比CVD风险为低度/未知的使用者更有可能停用ABC,无论病毒载量如何(≤1000拷贝/ml:相对率1.