Branche Angela R, Walsh Edward E, Jadhav Nagesh, Karmally Rachel, Baran Andrea, Peterson Derick R, Falsey Ann R
Department of Medicine, University of Rochester, Rochester, NY, United States of America.
Department of Medicine, Rochester General Hospital, Rochester, NY, United States of America.
PLoS One. 2016 Apr 4;11(4):e0152986. doi: 10.1371/journal.pone.0152986. eCollection 2016.
Lower respiratory tract illness (LRTI) frequently causes adult hospitalization and antibiotic overuse. Procalcitonin (PCT) treatment algorithms have been used successfully in Europe to safely reduce antibiotic use for LRTI but have not been adopted in the United States. We recently performed a feasibility study for a randomized clinical trial (RCT) of PCT and viral testing to guide therapy for non-pneumonic LRTI.
The primary objective of the current study was to understand factors influencing PCT algorithm adherence during the RCT and evaluate factors influencing provider antibiotic prescribing practices for LRTI.
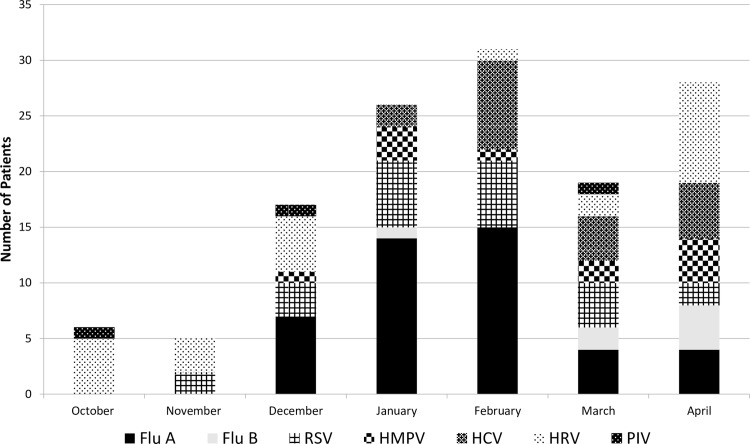
From October 2013-April 2014, 300 patients hospitalized at a community teaching hospital with non-pneumonic LRTI were randomized to standard or PCT-guided care with viral PCR testing. Algorithm adherence data was collected and multivariate stepwise logistic regression of clinical variables used to model algorithm compliance. 134 providers were surveyed anonymously before and after the trial to assess knowledge of biomarkers and viral testing and antibiotic prescribing practices.
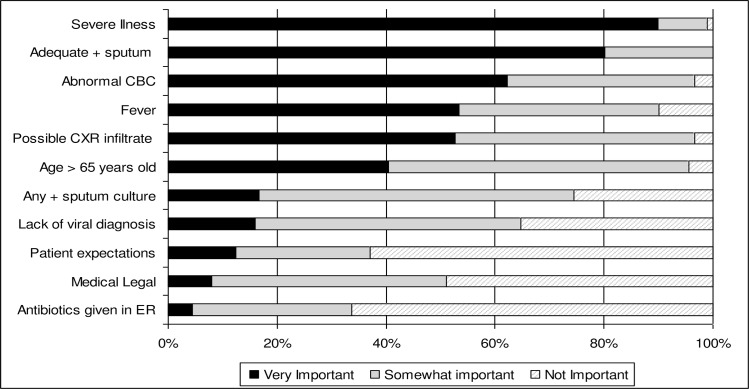
Diagnosis of pneumonia on admission was the only variable significantly associated with non-adherence [7% (adherence) vs. 26% (nonadherence), p = 0.01]. Surveys confirmed possible infiltrate on chest radiograph as important for provider decisions, as were severity of illness, positive sputum culture, abnormal CBC and fever. However, age, patient expectations and medical-legal concerns were also at least somewhat important to prescribing practices. Physician agreement with the importance of viral and PCT testing increased from 42% to 64% (p = 0.007) and 49% to 74% (p = 0.001), respectively, after the study.
Optimal algorithm adherence will be important for definitive PCT intervention trials in the US to determine if PCT guided algorithms result in better outcomes than reliance on traditional clinical variables. Factors influencing treatment decisions such as patient age, presence of fever, patient expectations and medical legal concerns may be amenable to education to improve PCT algorithm compliance for LRTI.
下呼吸道疾病(LRTI)常导致成人住院及抗生素过度使用。降钙素原(PCT)治疗方案已在欧洲成功应用,可安全减少LRTI的抗生素使用,但在美国尚未采用。我们最近进行了一项可行性研究,以开展一项关于PCT和病毒检测的随机临床试验(RCT),用于指导非肺炎性LRTI的治疗。
本研究的主要目的是了解随机临床试验期间影响PCT方案依从性的因素,并评估影响医疗服务提供者对LRTI抗生素处方行为的因素。
2013年10月至2014年4月,300名在社区教学医院因非肺炎性LRTI住院的患者被随机分为接受标准治疗或PCT指导治疗并进行病毒PCR检测。收集方案依从性数据,并对用于构建方案依从性模型的临床变量进行多因素逐步逻辑回归分析。在试验前后对134名医疗服务提供者进行匿名调查,以评估其对生物标志物和病毒检测的了解以及抗生素处方行为。
入院时诊断为肺炎是唯一与不依从显著相关的变量[依从率7%,不依从率26%,p = 0.01]。调查证实,胸部X线片上可能存在浸润对医疗服务提供者的决策很重要,疾病严重程度、痰培养阳性、血常规异常和发热也是如此。然而,年龄、患者期望和医疗法律问题对处方行为也至少有一定重要性。研究结束后,医生对病毒和PCT检测重要性的认同率分别从42%提高到64%(p = 0.007)和从49%提高到74%(p = 0.001)。
在美国,最佳方案依从性对于确定性PCT干预试验很重要,以确定PCT指导方案是否比依赖传统临床变量能带来更好的结果。影响治疗决策的因素,如患者年龄、发热情况、患者期望和医疗法律问题,可能可通过教育来改善LRTI的PCT方案依从性。